You might also like
- Maternal Diagnostic in 1ST Trimester 2022Document15 pagesMaternal Diagnostic in 1ST Trimester 2022Manoj DongarwarNo ratings yet
- Diagnostic Modalities in PregnancyDocument11 pagesDiagnostic Modalities in PregnancyRavina Patel100% (1)
- Diagnosis of PregnancyDocument26 pagesDiagnosis of PregnancyMounikaNo ratings yet
- Pregnancy Confirmation and ChangesDocument37 pagesPregnancy Confirmation and Changesana aurea aquino de leonNo ratings yet
- 68 Abnormal PeuperiumDocument44 pages68 Abnormal PeuperiumGodsonYeboah-AwudziNo ratings yet
- Diagnosisofpregnancy 150127223055 Conversion Gate01Document40 pagesDiagnosisofpregnancy 150127223055 Conversion Gate01madhu.BNo ratings yet
- 5-Dx of PregnancyDocument46 pages5-Dx of PregnancybenNo ratings yet
- MATERNAL AND CHILD HEALTH NURSINGDocument40 pagesMATERNAL AND CHILD HEALTH NURSINGTina Talmadge100% (5)
- Diagnosis of PregnancyDocument21 pagesDiagnosis of PregnancyNestaNo ratings yet
- Notes-Maternal Health NursingDocument22 pagesNotes-Maternal Health NursingRachael Crossgrove100% (4)
- Maternal and Child Health NursingDocument39 pagesMaternal and Child Health NursingRena VilNo ratings yet
- Infertility IIDocument58 pagesInfertility IIdr_asalehNo ratings yet
- (Text) Maternal and Child Health NursingDocument40 pages(Text) Maternal and Child Health NursingVia H.No ratings yet
- MCHN Reviewer 1Document24 pagesMCHN Reviewer 1Steam LcNo ratings yet
- DX of PregnancyDocument41 pagesDX of Pregnancyshivamg.sg1234No ratings yet
- Angrej Sir Obstetrics NotesssDocument119 pagesAngrej Sir Obstetrics Notessslakhwinder batthNo ratings yet
- Diagnosis of PregnancyDocument23 pagesDiagnosis of PregnancyNeelesh BhandariNo ratings yet
- Infertility - Definition, Causes, Diagnostic Procedures AND CouncellingDocument37 pagesInfertility - Definition, Causes, Diagnostic Procedures AND CouncellingvincentsharonNo ratings yet
- Antenatal CareDocument46 pagesAntenatal CareKIPA SHRESTHANo ratings yet
- 2 & 3.Biochemical Changes in PregnancyDocument23 pages2 & 3.Biochemical Changes in PregnancydeepaNo ratings yet
- DIAGNOSIS OF PREGNANCY SIGNSDocument58 pagesDIAGNOSIS OF PREGNANCY SIGNSpriyanka33% (3)
- Diagnosis of Pregnancy - Signs, Differential DiagnosisDocument39 pagesDiagnosis of Pregnancy - Signs, Differential DiagnosisKripa SusanNo ratings yet
- AntepartalDocument43 pagesAntepartalxing414No ratings yet
- AbortionDocument36 pagesAbortionAnjali Rahul AjmeriNo ratings yet
- Biochemical Methods ObgDocument25 pagesBiochemical Methods ObgRupali AroraNo ratings yet
- Pregnancy Diagnosis and Fetal AssessmentDocument41 pagesPregnancy Diagnosis and Fetal AssessmentKrystel Anne MilanNo ratings yet
- Signs Indicating Possible Complications of PregnancyDocument6 pagesSigns Indicating Possible Complications of Pregnancygerald polopotNo ratings yet
- Perub Fisik Saat KehamilanDocument66 pagesPerub Fisik Saat KehamilanrismaNo ratings yet
- Maternal and Child Health Nursing I: Pamantasan NG Lungsod NG MaynilaDocument39 pagesMaternal and Child Health Nursing I: Pamantasan NG Lungsod NG MaynilaFrAnz Angel Padera100% (1)
- Maternal and Child SemifinalsDocument31 pagesMaternal and Child SemifinalsKarl Symon AmperNo ratings yet
- Bab I1Document30 pagesBab I1Ana Abadi Al IndNo ratings yet
- New NORMAL PUERPERIUMDocument21 pagesNew NORMAL PUERPERIUMvarshaNo ratings yet
- Puerperium and Its Management 1Document35 pagesPuerperium and Its Management 1Elvis100% (2)
- Diagnosing Pregnancy in the First TrimesterDocument34 pagesDiagnosing Pregnancy in the First TrimesterSanjeet SahNo ratings yet
- ABORTIONDocument10 pagesABORTIONSivi Joseph100% (1)
- Clinical Activities: A. Pre - ConsultationDocument13 pagesClinical Activities: A. Pre - ConsultationerykafadsNo ratings yet
- Introduction to Neonatology at Kharkiv UniversityDocument47 pagesIntroduction to Neonatology at Kharkiv Universitysobhan fouladnezhadNo ratings yet
- Ob1 Lecture 1Document54 pagesOb1 Lecture 1Respia Leyson BandalaNo ratings yet
- Institute of Nursing Intrapartum Care Handouts: Labor and Delivery Theories of Labor OnsetDocument7 pagesInstitute of Nursing Intrapartum Care Handouts: Labor and Delivery Theories of Labor OnsetTimi BCNo ratings yet
- Puerperum Notes 1Document7 pagesPuerperum Notes 1Google SecurityNo ratings yet
- APMC CH 9Document3 pagesAPMC CH 9Jhessie ChingNo ratings yet
- Chap 8 Prenatal CareDocument10 pagesChap 8 Prenatal CareRem AlfelorNo ratings yet
- Fertilization To Conception: Maternal and Child Health Nursing PregnancyDocument8 pagesFertilization To Conception: Maternal and Child Health Nursing PregnancyNikki M. Arapol100% (1)
- Pregnancy Diagnosis StagesDocument25 pagesPregnancy Diagnosis StagesA suhasiniNo ratings yet
- MaternalDocument41 pagesMaternalUc_tweenNo ratings yet
- Normal PuerperiumDocument23 pagesNormal Puerperiumnaga maniNo ratings yet
- Changes During PregnancyDocument2 pagesChanges During PregnancyRalph Tama Mangacop BenitoNo ratings yet
- By Intern Dr. Borhan UddinDocument12 pagesBy Intern Dr. Borhan UddinmanjuNo ratings yet
- Gestational Conditions HandoutDocument17 pagesGestational Conditions HandoutFilamae Jayahr Caday100% (4)
- MENSTRUATION: Monthly Discharge of Blood From The Uterus Occurring Form Puberty To MenopauseDocument18 pagesMENSTRUATION: Monthly Discharge of Blood From The Uterus Occurring Form Puberty To Menopauselyka resurreccionNo ratings yet
- AbortionDocument35 pagesAbortionZahida Aida Ida Paramore100% (1)
- Abortion and Ectopic PregnancyDocument3 pagesAbortion and Ectopic PregnancyJefelson Eu Palaña NahidNo ratings yet
- History TakingDocument26 pagesHistory TakingShauie CayabyabNo ratings yet
- 208-230 CH08 Lowdermilk - QXD PDFDocument46 pages208-230 CH08 Lowdermilk - QXD PDFlalaNo ratings yet
- Signs of PregnancyDocument53 pagesSigns of PregnancyFrancr ToledanoNo ratings yet
- Abortion Definition, Types, Causes and ManagementDocument77 pagesAbortion Definition, Types, Causes and ManagementPadmaNo ratings yet
- Labor Monitoring and ManagementDocument2 pagesLabor Monitoring and ManagementFreakyRustlee LeoragNo ratings yet
- PT&T Policy Against Married WomenDocument12 pagesPT&T Policy Against Married WomenHershey Delos SantosNo ratings yet
- Anacardium OrientaleDocument21 pagesAnacardium OrientaleAlexandre Funcia100% (1)
- Key To Eye Diagnosis by Tashfeen NasiraDocument8 pagesKey To Eye Diagnosis by Tashfeen Nasiralakshay sharmaNo ratings yet
- Nursing Care Plan Hirschsprung's Disease (Congenital A Ganglionic Mega Colon)Document2 pagesNursing Care Plan Hirschsprung's Disease (Congenital A Ganglionic Mega Colon)deric87% (30)
- ROO-ALL-HS-PRO-0025 REV 10 Ground Disturbance and Excavation Procedure - ...Document25 pagesROO-ALL-HS-PRO-0025 REV 10 Ground Disturbance and Excavation Procedure - ...Murtadda MohammedNo ratings yet
- Acute Pain Questions - LathaDocument5 pagesAcute Pain Questions - LathaNishanth yedavalliNo ratings yet
- OCP - 15 - GrindingDocument2 pagesOCP - 15 - GrindingNagendra Kumar SinghNo ratings yet
- Videoke OrdinanceDocument3 pagesVideoke Ordinanceroland carub100% (2)
- Central Causes of DizzinessDocument9 pagesCentral Causes of DizzinessGLORIA MEDINA HERNANDEZNo ratings yet
- Job Description - Hardware OfficerDocument2 pagesJob Description - Hardware OfficerGuyana Red Cross SocietyNo ratings yet
- ABYIP-2023 TemplateDocument3 pagesABYIP-2023 Templatejomar88% (26)
- Histopathology: The Study of Disease at the Tissue LevelDocument5 pagesHistopathology: The Study of Disease at the Tissue LevelPau Basco75% (4)
- (ILM Super Series) Institute of Leadership & Mana - Caring For The Customer Super Series, Fourth Edition - Pergamon Flexible Learning (2002)Document117 pages(ILM Super Series) Institute of Leadership & Mana - Caring For The Customer Super Series, Fourth Edition - Pergamon Flexible Learning (2002)bankadhi100% (1)
- Spa CuisineDocument11 pagesSpa CuisineNamanraj Singh JollyNo ratings yet
- Drug Presentation On: Aminoven: Submitted To Submitted byDocument6 pagesDrug Presentation On: Aminoven: Submitted To Submitted byShilpi SinghNo ratings yet
- 849 FullDocument13 pages849 FullAnsuf WicaksonoNo ratings yet
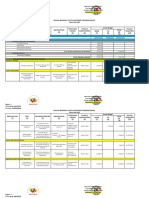
- Kauswagan Central Elementary promotes health and wellnessDocument31 pagesKauswagan Central Elementary promotes health and wellnessMayMay SaturNo ratings yet
- Exercise 3 - TRANSFER AND COLONY SELECTION TECHNIQUESDocument13 pagesExercise 3 - TRANSFER AND COLONY SELECTION TECHNIQUESArslan AmeenNo ratings yet
- Ds Pedia WardDocument2 pagesDs Pedia WardRhea Mae Valles - ReyesNo ratings yet
- Week 12-13-Group Activity-Conceptualizing A Possible GMODocument5 pagesWeek 12-13-Group Activity-Conceptualizing A Possible GMOAlexandra MandrezaNo ratings yet
- Hip ExaminationDocument7 pagesHip ExaminationWaqas Haleem100% (1)
- Strategies For Minimizing Dispensing ErrorsDocument3 pagesStrategies For Minimizing Dispensing ErrorsAnah MayNo ratings yet
- Pulmonary Atresia With An Intact Ventricular Septum: Preoperative Physiology, Imaging, and ManagementDocument11 pagesPulmonary Atresia With An Intact Ventricular Septum: Preoperative Physiology, Imaging, and ManagementAkilaNo ratings yet
- Gronning 2017 CloningDocument4 pagesGronning 2017 CloningKlyde Orly R. YusoresNo ratings yet
- Deeper Root Academy HandbookDocument18 pagesDeeper Root Academy HandbookAdminNo ratings yet
- Mapeh 10 Week 1 Week 2Document12 pagesMapeh 10 Week 1 Week 2Christian Paul YusiNo ratings yet
- Congestive Renal FailureDocument9 pagesCongestive Renal FailureSayf QisthiNo ratings yet
- Body PlethysmographyDocument52 pagesBody PlethysmographyppgpcsNo ratings yet
- RAPID Resources for Lowering Fertility and Achieving Sustainable Development in the PhilippinesDocument41 pagesRAPID Resources for Lowering Fertility and Achieving Sustainable Development in the PhilippinesLeyrra Paclibar DiduloNo ratings yet
- Reducing AgeismDocument2 pagesReducing AgeismAntónio LealNo ratings yet