You might also like
- Statistics - Probability - Q3 - Mod4 - Random Sampling, Parameter and StatisticDocument24 pagesStatistics - Probability - Q3 - Mod4 - Random Sampling, Parameter and StatisticSheebei Sheebei92% (26)
- Efficacy of Low-Level Laser Therapy in Carpal Tunnel Syndrome ManagementDocument10 pagesEfficacy of Low-Level Laser Therapy in Carpal Tunnel Syndrome ManagementChung Tze YangNo ratings yet
- Ayoub Jumanne Proposal MzumbeDocument36 pagesAyoub Jumanne Proposal MzumbeGoodluck Savutu Lucumay50% (2)
- Critical Appraisal of Journal Article - 5: BY DR - Gautam.G.J, Third Year PostgraduateDocument36 pagesCritical Appraisal of Journal Article - 5: BY DR - Gautam.G.J, Third Year PostgraduateGautam G JNo ratings yet
- Taborri 2016 (Review)Document20 pagesTaborri 2016 (Review)AFoqsdifNo ratings yet
- Models To Predict Cardiovascular Risk - Comparison of CART, Multilayer Perceptron and Logistic RegressionDocument5 pagesModels To Predict Cardiovascular Risk - Comparison of CART, Multilayer Perceptron and Logistic RegressionAbel DemelashNo ratings yet
- Final R PDocument22 pagesFinal R Pdisha groverNo ratings yet
- Dodge - Symposium MCI 2014 V5Document33 pagesDodge - Symposium MCI 2014 V5WorldEventsForumNo ratings yet
- Deep Forest Based Multivariate Classification For Diagnostic Health MonitoringDocument7 pagesDeep Forest Based Multivariate Classification For Diagnostic Health MonitoringranaNo ratings yet
- Psychological StatisticsDocument170 pagesPsychological StatisticsKarthick VijayNo ratings yet
- Loftus, Ian-Care of The Critically Ill Surgical Patient-Hodder Arnold (2010)Document4 pagesLoftus, Ian-Care of The Critically Ill Surgical Patient-Hodder Arnold (2010)benjielawNo ratings yet
- Steyerberg Prediction Modeling 7 Steps Jan10Document45 pagesSteyerberg Prediction Modeling 7 Steps Jan10Fajar Rudy QimindraNo ratings yet
- Meta Análisis Con RDocument14 pagesMeta Análisis Con R290971No ratings yet
- Report DiabeticsDocument8 pagesReport DiabeticsBindhu NNo ratings yet
- Dodge Symposium MCI 2014 V7 LatestDocument34 pagesDodge Symposium MCI 2014 V7 LatestWorldEventsForumNo ratings yet
- Medial Tibial Stress Syndrome in Novice and Recreational Runners: A Systematic ReviewDocument13 pagesMedial Tibial Stress Syndrome in Novice and Recreational Runners: A Systematic ReviewasdfssonNo ratings yet
- Synopsis Diabetes Pred System MLDocument9 pagesSynopsis Diabetes Pred System MLsaurav shekharNo ratings yet
- Báo KHDocument12 pagesBáo KHDUY VÕ HUỲNH NHẬTNo ratings yet
- MedicalBiostatistics3rdEd C00Document30 pagesMedicalBiostatistics3rdEd C00Yousuf MdNo ratings yet
- CONSORT 2001 ChecklistDocument2 pagesCONSORT 2001 ChecklistmuchanakbaeNo ratings yet
- 4 - 2020 - Acup para Reab Pós-Avc Trat Neglet Unilateral - Sist Rev + Meta AnalDocument9 pages4 - 2020 - Acup para Reab Pós-Avc Trat Neglet Unilateral - Sist Rev + Meta AnalLuis Miguel MartinsNo ratings yet
- Cho 2018Document12 pagesCho 2018moses1999.mmNo ratings yet
- Improvements in Gait Characteristics After Intensive Resistance and Functional Training in People With DementiaDocument9 pagesImprovements in Gait Characteristics After Intensive Resistance and Functional Training in People With DementiaJun Seok KimNo ratings yet
- International Journal of Computational Engineering Research (IJCER)Document4 pagesInternational Journal of Computational Engineering Research (IJCER)International Journal of computational Engineering research (IJCER)No ratings yet
- Chapter 2: MethodologyDocument9 pagesChapter 2: MethodologyDonna WilliamsNo ratings yet
- MCQ 2Document9 pagesMCQ 2Munni KNo ratings yet
- STARD 2015 Checklist-RSNADocument5 pagesSTARD 2015 Checklist-RSNAdoctoriyoNo ratings yet
- RCT CONSORT-Critical AppraisalDocument79 pagesRCT CONSORT-Critical AppraisalamaliaNo ratings yet
- Thyroid Disease PredictionDocument44 pagesThyroid Disease PredictionshanmukhaadityavenkatNo ratings yet
- John Moult, Krzysztof Fidelis, CASPDocument4 pagesJohn Moult, Krzysztof Fidelis, CASPAnkita SinghNo ratings yet
- Accelerometer Data Collection and Processing Criteria To AssessDocument25 pagesAccelerometer Data Collection and Processing Criteria To AssessBJNo ratings yet
- Wearable Sensors For Clinical Applications in Epilepsy, Parkinson's Disease, and Stroke: A Mixed Methods Systematic ReviewDocument13 pagesWearable Sensors For Clinical Applications in Epilepsy, Parkinson's Disease, and Stroke: A Mixed Methods Systematic ReviewMANIMEGALAI M. ECENo ratings yet
- Exercise Training Modalities For Heart Transplant Recipients. A Systematic Review and Network Meta-Analysis ProtocolDocument6 pagesExercise Training Modalities For Heart Transplant Recipients. A Systematic Review and Network Meta-Analysis ProtocolNelson Carvas JrNo ratings yet
- Predicting and Detection of Heart Disease Using MachineDocument20 pagesPredicting and Detection of Heart Disease Using Machinestudent lifeNo ratings yet
- Predicting and Detection of Heart Disease Using MachineDocument20 pagesPredicting and Detection of Heart Disease Using Machinestudent lifeNo ratings yet
- Irjet V5i4896 PDFDocument4 pagesIrjet V5i4896 PDFM. Talha NadeemNo ratings yet
- Author Response 5.4.19Document28 pagesAuthor Response 5.4.19sakthithirumaraiNo ratings yet
- Evaluación Clínica y Funcional Del HombroDocument9 pagesEvaluación Clínica y Funcional Del HombroLuis Eduardo Cabezas MirandaNo ratings yet
- Improving Oncology Trials Through Adaptive Trial Design - ACT-Oncology-eBook-2016-MayDocument7 pagesImproving Oncology Trials Through Adaptive Trial Design - ACT-Oncology-eBook-2016-MayRaviprakash MadhyasthaNo ratings yet
- Bo Hannon 2016Document5 pagesBo Hannon 2016rafaelorcyNo ratings yet
- 2nd Christo Journal Club PresentationDocument19 pages2nd Christo Journal Club Presentationchristo sebastianNo ratings yet
- GUID - 5 en-USDocument29 pagesGUID - 5 en-USAndrés Ignacio Solano SeravalliNo ratings yet
- Relatório Revisão Sistemática Com Metanálise PDFDocument30 pagesRelatório Revisão Sistemática Com Metanálise PDFValéria CruzNo ratings yet
- Official: Á1010Ñ Analytical Data-Interpretation and TreatmentDocument29 pagesOfficial: Á1010Ñ Analytical Data-Interpretation and TreatmentDilawar BakhtNo ratings yet
- Early Alzheimer's Disease Prediction in Machine Learning Setup: Empirical Analysis With Missing Value ComputationDocument8 pagesEarly Alzheimer's Disease Prediction in Machine Learning Setup: Empirical Analysis With Missing Value Computationqurat ul ain annieNo ratings yet
- Captura de Tela 2023-04-15 À(s) 08.50.03Document13 pagesCaptura de Tela 2023-04-15 À(s) 08.50.03Daiana BündchenNo ratings yet
- Clinical Gait Assessment in The Neurologically ImpairedDocument6 pagesClinical Gait Assessment in The Neurologically Impairedvamat63No ratings yet
- Comprehensive Literature Review and Statistical Considerations For Microarray Meta-AnalysisDocument6 pagesComprehensive Literature Review and Statistical Considerations For Microarray Meta-Analysisea442225No ratings yet
- ML ReportDocument12 pagesML ReportPrakhar AroraNo ratings yet
- Writing Statistical Section and Presentation of Results - Juliana NamutunduDocument37 pagesWriting Statistical Section and Presentation of Results - Juliana NamutunduDr.Turyagumanawe JohnNo ratings yet
- Laboratory 10Document8 pagesLaboratory 10tina m fayzaNo ratings yet
- Prediction of Diabetes Disease Using Machine Learning Algorithms28 20782Document7 pagesPrediction of Diabetes Disease Using Machine Learning Algorithms28 20782IAES IJAINo ratings yet
- Research Paper 2023Document28 pagesResearch Paper 202307ABHISHEK MISHRANo ratings yet
- Research Article Automated Atrial Fibrillation Detection Based On Feature Fusion Using Discriminant Canonical Correlation AnalysisDocument10 pagesResearch Article Automated Atrial Fibrillation Detection Based On Feature Fusion Using Discriminant Canonical Correlation Analysisaryelit velardesNo ratings yet
- Deep Learning For Healthcare Applications Based On Physiological Signals: A ReviewDocument31 pagesDeep Learning For Healthcare Applications Based On Physiological Signals: A ReviewGoutam AgrawalNo ratings yet
- Individual Participant DataDocument18 pagesIndividual Participant DataSajjad alipourNo ratings yet
- Module 1 EE Data AnalysisDocument13 pagesModule 1 EE Data AnalysisClint Mosenabre100% (1)
- Jassal Et Al. - 2023 - Artificial Intelligence For Pre-Operative DiagnosisDocument10 pagesJassal Et Al. - 2023 - Artificial Intelligence For Pre-Operative DiagnosisJamesLeeNo ratings yet
- Information: A Heart Disease Prediction Model Based On Feature Optimization and Smote-Xgboost AlgorithmDocument15 pagesInformation: A Heart Disease Prediction Model Based On Feature Optimization and Smote-Xgboost Algorithmharshitvashisth76No ratings yet
- Huang Meta Analyses Stat Methods Med Res 2014 0962280214537394Document35 pagesHuang Meta Analyses Stat Methods Med Res 2014 0962280214537394Habib MradNo ratings yet
- CommaDocument18 pagesCommaMunna KendreNo ratings yet
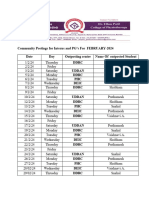
- Community Postings For PG (Feb 2024)Document2 pagesCommunity Postings For PG (Feb 2024)Munna KendreNo ratings yet
- Adobe Scan 08 Dec 2023Document6 pagesAdobe Scan 08 Dec 2023Munna KendreNo ratings yet
- PDF World URD - Circular No - 02 State Level Research Competition - 180124Document8 pagesPDF World URD - Circular No - 02 State Level Research Competition - 180124Munna KendreNo ratings yet
- Introduction To Research MethodologyDocument20 pagesIntroduction To Research MethodologyMunna KendreNo ratings yet
- CP AssessmentDocument10 pagesCP AssessmentMunna KendreNo ratings yet
- Push 3Document2 pagesPush 3Sandeep SharmaNo ratings yet
- Summer 2016 To Winter 2018 Advance in Neurophysiotherapy (Part-II) - IVDocument6 pagesSummer 2016 To Winter 2018 Advance in Neurophysiotherapy (Part-II) - IVMunna KendreNo ratings yet
- Snehal JCDocument32 pagesSnehal JCMunna KendreNo ratings yet
- Vaishnavi JC FinalDocument21 pagesVaishnavi JC FinalMunna KendreNo ratings yet
- Excel 20230617 123520Document9 pagesExcel 20230617 123520Munna KendreNo ratings yet
- Shubham New 66Document49 pagesShubham New 66Munna KendreNo ratings yet
- Gayatri ProjectDocument44 pagesGayatri ProjectMunna KendreNo ratings yet
- Choosing Safe and Suitable Bicycle Routes To Integrate Cycling andDocument17 pagesChoosing Safe and Suitable Bicycle Routes To Integrate Cycling andAntonio Aldo RamirezNo ratings yet
- Effect of Parental Involvement On The Reading Skills of Pupils in Lower Primary School in Ondo State, NigeriaDocument8 pagesEffect of Parental Involvement On The Reading Skills of Pupils in Lower Primary School in Ondo State, NigeriaTeresa Mae Abuzo Vallejos-BucagNo ratings yet
- Chapter 5Document2 pagesChapter 5Lourene Jauod- GuanzonNo ratings yet
- Chapter 2 - 1 - Roots of Equations - Bracketing MethodsDocument24 pagesChapter 2 - 1 - Roots of Equations - Bracketing MethodsRoger FernandezNo ratings yet
- Comparative Analysis On Perceived Service Quality of Banks and Non-Banking Financial Companies (NBFCS) - Evidence From Commercial Vehicle FinanceDocument6 pagesComparative Analysis On Perceived Service Quality of Banks and Non-Banking Financial Companies (NBFCS) - Evidence From Commercial Vehicle FinanceLaxman NayakNo ratings yet
- COMP616 STAT604 Assignment 1 QuestionsDocument5 pagesCOMP616 STAT604 Assignment 1 Questionsapsno233No ratings yet
- C - Proposal ResearchDocument30 pagesC - Proposal ResearchNawaraj GhimireNo ratings yet
- Permission To Conduct Research ExamplesDocument2 pagesPermission To Conduct Research ExamplesVincent MaspilNo ratings yet
- The Technology Acceptance Model: January 2008Document15 pagesThe Technology Acceptance Model: January 2008إمحمد السنوسي القزيريNo ratings yet
- 4final REPORT - 1-62Document64 pages4final REPORT - 1-62Jyoti YadavNo ratings yet
- SRMDocument6 pagesSRMsidharthNo ratings yet
- Boddy 2016Document8 pagesBoddy 2016EBO The InspirationistNo ratings yet
- Research Process Notes PDFDocument18 pagesResearch Process Notes PDFCLAUDINE MUGABEKAZINo ratings yet
- 4024 w12 QP 21Document24 pages4024 w12 QP 21Beatrice RossNo ratings yet
- RM Notes (5modules)Document136 pagesRM Notes (5modules)rihan786mr7No ratings yet
- Parts of A Research Report - 2018Document104 pagesParts of A Research Report - 2018GINABELLE COLIMA100% (1)
- Basics of Statistical Inference: Drawing Inferences From A Starbucks SurveyDocument28 pagesBasics of Statistical Inference: Drawing Inferences From A Starbucks SurveyDipesh MundhraNo ratings yet
- Research Methodology by C.R.kothariDocument11 pagesResearch Methodology by C.R.kothariBala Subramaniyam50% (2)
- 96BDocument3 pages96BJamie SchultzNo ratings yet
- Data CollectionDocument3 pagesData CollectionRHoDY PRODUCTIONSNo ratings yet
- Cingeletal COiPDocument21 pagesCingeletal COiPMakanudo.No ratings yet
- Module 1 Activity - Basic Concepts in IOP PDFDocument2 pagesModule 1 Activity - Basic Concepts in IOP PDFJessie JuliaNo ratings yet
- A Complete Guide To Survival Analysis in Python, Part 3 - KDnuggetsDocument22 pagesA Complete Guide To Survival Analysis in Python, Part 3 - KDnuggets8c354be21dNo ratings yet
- NMIMS Semester 2 Assignment Solution June 2021 Call 9025810064Document8 pagesNMIMS Semester 2 Assignment Solution June 2021 Call 9025810064Palaniappan NNo ratings yet
- TFM Ferespe CarolinaGuimaraes FINALDocument60 pagesTFM Ferespe CarolinaGuimaraes FINALAdnanNo ratings yet
- Soilworks For Structural EngineersDocument4 pagesSoilworks For Structural EngineersAshish LoyaNo ratings yet
- ThesisDocument47 pagesThesisAhmad MahmoodNo ratings yet
- Business Research Report TemplateDocument40 pagesBusiness Research Report TemplateJessy YeNo ratings yet