You might also like
- Handbook of Surgical Care For House OfficersDocument22 pagesHandbook of Surgical Care For House OfficersDeep SleepNo ratings yet
- Power Point Consumer Health EducationDocument81 pagesPower Point Consumer Health EducationLovelyn Calaramo Bello91% (23)
- Your Body Believes Every Word Y - Barbara Hoberman LevineDocument380 pagesYour Body Believes Every Word Y - Barbara Hoberman LevineRoryBradshawNo ratings yet
- Risk Assessment: AS A GradingDocument12 pagesRisk Assessment: AS A GradingNAGARAJNo ratings yet
- Anestesi Abdominal ApproachDocument14 pagesAnestesi Abdominal ApproachabdulkadirmunsyNo ratings yet
- Surgical Infections Chapter 5 Shcwartz Principles of SurgeryDocument34 pagesSurgical Infections Chapter 5 Shcwartz Principles of Surgeryanas hindawi100% (4)
- VesicolithotomyDocument14 pagesVesicolithotomyMico Ga Bisa GendutNo ratings yet
- Operating Room TeamDocument18 pagesOperating Room TeamKatrina PonceNo ratings yet
- Perforative PeritonitisDocument58 pagesPerforative PeritonitisSangeeta BSR82% (17)
- Timing of Surgery in Infectious EndocarditisDocument3 pagesTiming of Surgery in Infectious EndocarditisBejan George BogdanNo ratings yet
- Preoperative Evaluation For Non-Cardiac Surgery: AK GhoshDocument6 pagesPreoperative Evaluation For Non-Cardiac Surgery: AK GhoshAshvanee Kumar SharmaNo ratings yet
- 2014 AHA SummaryDocument14 pages2014 AHA SummaryiamseraNo ratings yet
- Intro To Postop ComplicationsDocument11 pagesIntro To Postop ComplicationsRobert UntaruNo ratings yet
- Management of Common PostoperativeComplicationsDocument15 pagesManagement of Common PostoperativeComplicationsjamalNo ratings yet
- ESC 2020 Infective Endocarditis and Neurologic Events - Indications and Timing For Surgical InterventionsDocument8 pagesESC 2020 Infective Endocarditis and Neurologic Events - Indications and Timing For Surgical InterventionsJeffry HaryantoNo ratings yet
- Venousthromboembolism Andpulmonaryembolism: Strategies For Prevention and ManagementDocument14 pagesVenousthromboembolism Andpulmonaryembolism: Strategies For Prevention and ManagementDamian CojocaruNo ratings yet
- Infective EndocarditisDocument8 pagesInfective EndocarditissalahoveNo ratings yet
- Preoperative Preparation For Surgery: Presented By: Dr. Md. Mujibur Rahman Rony IMO, Ward: 24, Surgery Unit: 1 CMCHDocument31 pagesPreoperative Preparation For Surgery: Presented By: Dr. Md. Mujibur Rahman Rony IMO, Ward: 24, Surgery Unit: 1 CMCHginasti keistouNo ratings yet
- Abdomen TraumaDocument74 pagesAbdomen TraumajeevanNo ratings yet
- Essential Messages - 2023 EndocarditisDocument12 pagesEssential Messages - 2023 Endocarditisimran karimNo ratings yet
- Bernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?Document26 pagesBernard D. Prendergast and Pilar Tornos: Surgery For Infective Endocarditis: Who and When?om mkNo ratings yet
- Surgery & Aids: Prof - Amarjit Singh Lukram ImphalDocument49 pagesSurgery & Aids: Prof - Amarjit Singh Lukram ImphalDr L Amarjit SinghNo ratings yet
- Chapter 28 Management of Patients With StructuralDocument23 pagesChapter 28 Management of Patients With StructuralAbel C. Idusma Jr.No ratings yet
- ERCP BleedingDocument10 pagesERCP BleedingSamantha Florendo TinsayNo ratings yet
- Abdominal TraumaDocument59 pagesAbdominal TraumaEirene Sophie Wutoy HallatuNo ratings yet
- Anesthesia and Perioperative Management of Colorectal Surgical Patients - Specific Issues (Part 2)Document10 pagesAnesthesia and Perioperative Management of Colorectal Surgical Patients - Specific Issues (Part 2)Syauqi DarussalamNo ratings yet
- In Feccio NesDocument6 pagesIn Feccio NesCarla Cecilia UlloaNo ratings yet
- Early Ambulation and Prevention of Post-Operative Thrombo-Embolic RiskDocument4 pagesEarly Ambulation and Prevention of Post-Operative Thrombo-Embolic RiskAnderson LondoñoNo ratings yet
- Pre and Post Operative Care: To: DR - Biniyam. By: Biniam.MDocument56 pagesPre and Post Operative Care: To: DR - Biniyam. By: Biniam.MBini JaminNo ratings yet
- Endocarditis Nature 1Document13 pagesEndocarditis Nature 1NAREN FAVIAN BRAVO BRAVONo ratings yet
- Pre and Post Operative Care: To: DR - Biniyam.G By: Biniam.MDocument55 pagesPre and Post Operative Care: To: DR - Biniyam.G By: Biniam.MBini JaminNo ratings yet
- Post-Operative Wound Complications Following Emergency and Elective Abdominal SurgeriesDocument6 pagesPost-Operative Wound Complications Following Emergency and Elective Abdominal SurgeriesNurul Aini DamayantiNo ratings yet
- Quality Guidelines IVC FilterDocument9 pagesQuality Guidelines IVC Filteramrit koiralaNo ratings yet
- Prophylaxis of Infective Is Current Tendencies and Continuing Controversies Lancet 2008Document8 pagesProphylaxis of Infective Is Current Tendencies and Continuing Controversies Lancet 2008Dra BeleQueen Hernandez RodriguezNo ratings yet
- RVM y MedistinitisDocument5 pagesRVM y MedistinitisMartha CeciliaNo ratings yet
- Perioperative Appraoch To HIV ABdominal EmergencyDocument3 pagesPerioperative Appraoch To HIV ABdominal EmergencyKing-Iza CarrNo ratings yet
- Infective Endocarditis: History & ExamDocument75 pagesInfective Endocarditis: History & ExamMicija CucuNo ratings yet
- Chapter 28: Management of Patients With Structural, Infectious, and Inflammatory Cardiac DisordersDocument19 pagesChapter 28: Management of Patients With Structural, Infectious, and Inflammatory Cardiac DisordersBrian BileckyNo ratings yet
- Violation of Water-Electric Exchange in Patients With Nospecific Ulcerative Colitis Before Total ColectomyDocument5 pagesViolation of Water-Electric Exchange in Patients With Nospecific Ulcerative Colitis Before Total ColectomyIJRASETPublicationsNo ratings yet
- Diverticulitis TratamientoDocument4 pagesDiverticulitis TratamientoIván TorresNo ratings yet
- Complications After Free Ap Surgery: Do We Need A Standardized Classification of Surgical Complications?Document6 pagesComplications After Free Ap Surgery: Do We Need A Standardized Classification of Surgical Complications?drpuneetjindalNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument5 pagesAnnals of Medicine and Surgery: SciencedirectMishel Rodriguez GuzmanNo ratings yet
- 18 Infective EndocarditisDocument15 pages18 Infective EndocarditisCabdiNo ratings yet
- Vte Clinical Update Final - 190207 - 1 - LR FinalDocument6 pagesVte Clinical Update Final - 190207 - 1 - LR FinalSantosh SinghNo ratings yet
- Ehab 898Document9 pagesEhab 898Angelica Gaitan PalenciaNo ratings yet
- Endocarditis in The Intensive Care Unit An UpdateDocument10 pagesEndocarditis in The Intensive Care Unit An Updatecarper454No ratings yet
- Anesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFDocument11 pagesAnesthesia Management of Ophthalmic Surgery in Geriatric Patients PDFtiaraleshaNo ratings yet
- Uveitis and Systemic DiseasesDocument50 pagesUveitis and Systemic DiseasesAnumeha JindalNo ratings yet
- Infection and SIRS, AntibioticsDocument24 pagesInfection and SIRS, AntibioticsDaniel LimNo ratings yet
- Chiu 2015Document7 pagesChiu 2015retta tataNo ratings yet
- Establish A Perioperative Check Forum For Peripheral Intravenous Access To Prevent The Occurrence of PhlebitisDocument7 pagesEstablish A Perioperative Check Forum For Peripheral Intravenous Access To Prevent The Occurrence of Phlebitismohamad malikul mulkiNo ratings yet
- Postoperative Complications and ManagementDocument83 pagesPostoperative Complications and ManagementAditya Arya PutraNo ratings yet
- Total Abdominal Hysterectomy in A Patient With I 2024 International JournalDocument3 pagesTotal Abdominal Hysterectomy in A Patient With I 2024 International JournalRonald QuezadaNo ratings yet
- Preoreoperative Cardiac AssessmentDocument71 pagesPreoreoperative Cardiac AssessmentHossam atefNo ratings yet
- Daftar PustakaDocument6 pagesDaftar PustakaMeta ArindaNo ratings yet
- Pi Is 1078588417304057Document8 pagesPi Is 1078588417304057Dede MarizalNo ratings yet
- Postoperative ComplicationsDocument5 pagesPostoperative ComplicationsAhmed KanemazeNo ratings yet
- Atm 08 23 1626Document12 pagesAtm 08 23 1626Susana MalleaNo ratings yet
- Wound Infections inDocument6 pagesWound Infections inprissyben17No ratings yet
- 1.7 Right Person, Right Place, Right Time PDFDocument3 pages1.7 Right Person, Right Place, Right Time PDFKaren Osorio GilardiNo ratings yet
- Surgical-Site Infections Within 60 Days of Coronary Artery By-Pass Graft SurgeryDocument11 pagesSurgical-Site Infections Within 60 Days of Coronary Artery By-Pass Graft SurgeryMartha CeciliaNo ratings yet
- Diverticulita Cu Aer OlandaDocument6 pagesDiverticulita Cu Aer OlandacNo ratings yet
- International Journal of SurgeryDocument6 pagesInternational Journal of SurgeryM Ali AdrianNo ratings yet
- Perioperative Care of The Child: A Nursing Manual: October 2010 Vol 92 No4Document2 pagesPerioperative Care of The Child: A Nursing Manual: October 2010 Vol 92 No4Pahang Reforansa PutraNo ratings yet
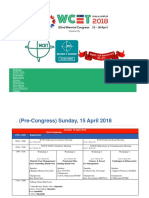
- Jadwal Wcet 2018 Kuala LumpurDocument36 pagesJadwal Wcet 2018 Kuala Lumpursunandar fatwaNo ratings yet
- Alexanders Surgical Procedures 1st Edition Rothrock Test BankDocument24 pagesAlexanders Surgical Procedures 1st Edition Rothrock Test Bankbraiding.apodanr4r465100% (33)
- Iso 11810 2015 en PDFDocument11 pagesIso 11810 2015 en PDFSuprio KamalNo ratings yet
- Coccygectomy Z PlastyDocument5 pagesCoccygectomy Z PlastyJayesh BhanushaliNo ratings yet
- 3 National Burn Management GuidelineDocument28 pages3 National Burn Management GuidelineNEsreNo ratings yet
- Ee System Messaging Brochure 0821Document8 pagesEe System Messaging Brochure 0821Jayjeet BhoiteNo ratings yet
- Biodata April2009Document12 pagesBiodata April2009drvithalkNo ratings yet
- NCM 112 Periop QuizletDocument13 pagesNCM 112 Periop QuizletZhoey ReyesNo ratings yet
- Obsidian Blades in Contemporary SurgeryDocument5 pagesObsidian Blades in Contemporary SurgerydrgrbicNo ratings yet
- Rosehip OilDocument2 pagesRosehip OilTy VoNo ratings yet
- Femoral Neck Fractures in Young Patients State Of.3Document5 pagesFemoral Neck Fractures in Young Patients State Of.3Rizwan Ahamed T ANo ratings yet
- The Effect of Hand Massage On Preoperative Anxiety in Ambulatory Surgery PatientsDocument10 pagesThe Effect of Hand Massage On Preoperative Anxiety in Ambulatory Surgery PatientsLia AgustinNo ratings yet
- Surgical CountsDocument17 pagesSurgical Countssubibabu1995No ratings yet
- My First Visit To KosovaDocument10 pagesMy First Visit To KosovaFjala e LireNo ratings yet
- Congenital Talipes Equino-Varus (Congenital Clubfoot) : Prof. Sohail Iqbal Sheikh Hod/Orthopaedics Iimct/PrhDocument66 pagesCongenital Talipes Equino-Varus (Congenital Clubfoot) : Prof. Sohail Iqbal Sheikh Hod/Orthopaedics Iimct/Prhawaisjinnah100% (1)
- Menieres-Slides 061213Document50 pagesMenieres-Slides 061213ajikwaNo ratings yet
- H. Tell Us Your Story Blank FormDocument6 pagesH. Tell Us Your Story Blank FormSophie Grace GriffinNo ratings yet
- Self Debriefing Questions - Vsim Week 5Document3 pagesSelf Debriefing Questions - Vsim Week 5api-631170779No ratings yet
- 2018 Consumer Survey On Digital Health: Us ResultsDocument17 pages2018 Consumer Survey On Digital Health: Us ResultsAcho DoradoNo ratings yet
- FHO DischargeDocument1 pageFHO DischargeVarghese NellimoottilNo ratings yet
- Pediatric Neuroanesthesia.3Document4 pagesPediatric Neuroanesthesia.3Mae Importers IncNo ratings yet
- Andra Prima Company Profile August19Document14 pagesAndra Prima Company Profile August19Monalisa ArmaniNo ratings yet
- Aendicus 3 UpdateDocument13 pagesAendicus 3 Updatetam meiNo ratings yet