You might also like
- The Pathology of Acute Myocardial Infarction: Patrick J GallagherDocument34 pagesThe Pathology of Acute Myocardial Infarction: Patrick J GallagherAlfun IqbalNo ratings yet
- Janos Gal Anaesthesia For The Cardiac Patient For Non Cardiac SurgeryDocument24 pagesJanos Gal Anaesthesia For The Cardiac Patient For Non Cardiac SurgeryParvathy R NairNo ratings yet
- Acute Coronay Syndrome - BACCDocument72 pagesAcute Coronay Syndrome - BACCYeyen Devyanti HandokoNo ratings yet
- Surgical Coronary Revascularization Who, What, WhenDocument68 pagesSurgical Coronary Revascularization Who, What, WhenAlaaGaballaNo ratings yet
- Ucm 484611Document92 pagesUcm 484611jackytungadiNo ratings yet
- Impact of Atropine and Aminophylline On TAVB With Inferior Wall MIDocument2 pagesImpact of Atropine and Aminophylline On TAVB With Inferior Wall MIRakhmat RamadhaniNo ratings yet
- Abubakar Zubeidi MCVU 2020Document22 pagesAbubakar Zubeidi MCVU 2020annisNo ratings yet
- CapricornDocument6 pagesCapricornMarkanthony256No ratings yet
- Cardiac ResuscitationDocument24 pagesCardiac ResuscitationPaulinaNo ratings yet
- 6 Hemorrhagic StrokeDocument54 pages6 Hemorrhagic StrokeErwinNo ratings yet
- ESC-2023 Day 3 UpdatesDocument41 pagesESC-2023 Day 3 UpdatesIvan TeongNo ratings yet
- Cardiogenic Shock: Updated Approach To ManagementDocument49 pagesCardiogenic Shock: Updated Approach To ManagementelsarahmiNo ratings yet
- Pre-Operative Assessment of Cardiac Patients in Non Cardiac SurgeryDocument36 pagesPre-Operative Assessment of Cardiac Patients in Non Cardiac SurgeryKush SurejaNo ratings yet
- 3.preoperative Patient Assessment and ManagementDocument76 pages3.preoperative Patient Assessment and Managementoliyad alemayehuNo ratings yet
- J Interven Cardiol. 2017 1-7.: Presented By: Dr. Yusrina BR Saragih Supervisor: DR - Dr. Zulfikri Mukhtar, Sp. JP (K)Document24 pagesJ Interven Cardiol. 2017 1-7.: Presented By: Dr. Yusrina BR Saragih Supervisor: DR - Dr. Zulfikri Mukhtar, Sp. JP (K)Yusrina Njoes SaragihNo ratings yet
- 1 s2.0 S0303846722004218 MainDocument7 pages1 s2.0 S0303846722004218 MainYULISSA FLORES RONDONNo ratings yet
- Admission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailureDocument18 pagesAdmission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailurePuja Nastia LubisNo ratings yet
- Edited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoDocument26 pagesEdited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoFikriYTNo ratings yet
- 2019 Enls For ApacvsnnnnnnDocument46 pages2019 Enls For ApacvsnnnnnnAhmed ElshewiNo ratings yet
- HicksCodeStrokeHospitalists PDFDocument57 pagesHicksCodeStrokeHospitalists PDFRizky DimasaputraNo ratings yet
- DR Vito Vascular ApicdDocument32 pagesDR Vito Vascular ApicdluckyariadneeNo ratings yet
- Acute Miocard InfarkDocument32 pagesAcute Miocard InfarkhansNo ratings yet
- Preanesthetic Assessment of Cardiac Patients UndDocument42 pagesPreanesthetic Assessment of Cardiac Patients UndParvathy R NairNo ratings yet
- Emergency MedicineDocument28 pagesEmergency Medicineshilpa sekhar278No ratings yet
- Presentasi Slide TerakhirDocument15 pagesPresentasi Slide TerakhirPutriNurulMuthiaNo ratings yet
- Circulation 1975 Burggraf 146 56Document12 pagesCirculation 1975 Burggraf 146 56Zikri Putra Lan LubisNo ratings yet
- Pereira Et Al-2016-Jornal Vascular Brasileiro - Sup-1Document5 pagesPereira Et Al-2016-Jornal Vascular Brasileiro - Sup-1carmenNo ratings yet
- Cerebral Microbleeds EditedDocument27 pagesCerebral Microbleeds EditedntuthukomkhabelaNo ratings yet
- High Total Leukocyte Count and Heart Failure After Myocardial InfarctionDocument10 pagesHigh Total Leukocyte Count and Heart Failure After Myocardial InfarctionRJMNo ratings yet
- 5 Week PracticeDocument60 pages5 Week PracticeKouka MahfoudiNo ratings yet
- Hemodynamic Monitoring in Cardiogenic Shock: ReviewDocument6 pagesHemodynamic Monitoring in Cardiogenic Shock: ReviewLeyden Chavez VergaraNo ratings yet
- Coronary Angiography and AngioplastyDocument24 pagesCoronary Angiography and AngioplastySemina Gazepi100% (2)
- Anaesthetic Implications of Common Congenital Heart ConditionsDocument56 pagesAnaesthetic Implications of Common Congenital Heart ConditionsShehan WijayasiriwardanaNo ratings yet
- Learner Cardiogenic Shock Secondary To Acute Myocardial InfarctionDocument5 pagesLearner Cardiogenic Shock Secondary To Acute Myocardial InfarctionHailee YakishNo ratings yet
- Cardiac Surgery Coronary I e IIDocument43 pagesCardiac Surgery Coronary I e IIFrancisNo ratings yet
- Chronic Stable Coronary DiseaseDocument63 pagesChronic Stable Coronary DiseaseAbnet WondimuNo ratings yet
- 4 - Acute STEMI With Cardiogenic ShockDocument18 pages4 - Acute STEMI With Cardiogenic ShockNiramol WeerasunthornNo ratings yet
- Comparison of Clinical Diagnosis With Computed Tomography in Ascertaining Type of StrokeDocument3 pagesComparison of Clinical Diagnosis With Computed Tomography in Ascertaining Type of StrokeDyah Wulan RamadhaniNo ratings yet
- Comparison of In-Hospital Outcome of Acute ST Elevation Myocardial Infarction in Patients With Versus Without Diabetes MellitusDocument7 pagesComparison of In-Hospital Outcome of Acute ST Elevation Myocardial Infarction in Patients With Versus Without Diabetes MellitusEsther DiazNo ratings yet
- Stemi 2Document51 pagesStemi 2Maryam MartawigunaNo ratings yet
- Management of IHD: Prepared By: Mohd Faizal Nizam Bin Mohd FoziDocument21 pagesManagement of IHD: Prepared By: Mohd Faizal Nizam Bin Mohd FoziMuazam ShahNo ratings yet
- Admission Vs Discharge Low Probability Chest PainDocument36 pagesAdmission Vs Discharge Low Probability Chest PainanggrainiNo ratings yet
- Stroke Simpo Perawat Dan AkupunturDocument54 pagesStroke Simpo Perawat Dan Akupunturaisyah nadhiraNo ratings yet
- Jurding BTKV AliDocument31 pagesJurding BTKV AliGani ArlondNo ratings yet
- Cardiogenic Shock - FINALDocument79 pagesCardiogenic Shock - FINALIgor StefanetNo ratings yet
- Acs UpdateDocument64 pagesAcs Updatekamel6No ratings yet
- 3745 PDFDocument6 pages3745 PDFJanuar RezkyNo ratings yet
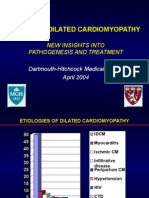
- Idiopathic Dilated Cardiomyopathy: New Insights Into Pathogenesis and TreatmentDocument51 pagesIdiopathic Dilated Cardiomyopathy: New Insights Into Pathogenesis and TreatmentAlexandra PataNo ratings yet
- Ucm 488377Document97 pagesUcm 488377Ahmad FahroziNo ratings yet
- Disease of The Coronary ArteriesDocument46 pagesDisease of The Coronary ArteriesDagimNo ratings yet
- Overview of The Acute Management of ST-elevation Myocardial InfarctionDocument28 pagesOverview of The Acute Management of ST-elevation Myocardial InfarctionAlice VoNo ratings yet
- ECG Case Studies Moosa1.Document54 pagesECG Case Studies Moosa1.m.ikhsan.adi.nugrahaNo ratings yet
- Cardiac TransplantDocument135 pagesCardiac TransplantNakka SrikanthNo ratings yet
- Episode 163 Acute Heart Failure Part 1Document8 pagesEpisode 163 Acute Heart Failure Part 1Dk YadavNo ratings yet
- Acquired Heart Disease EditedDocument63 pagesAcquired Heart Disease Editedapalah_niNo ratings yet
- Acquired Heart Disease Edited2Document50 pagesAcquired Heart Disease Edited2apalah_niNo ratings yet
- Acute Coronary SyndrommeDocument50 pagesAcute Coronary SyndrommeAndriani Kemala SariNo ratings yet
- JournalpresentDocument32 pagesJournalpresentteddyporNo ratings yet
- Diercks 2006Document6 pagesDiercks 2006koasspyNo ratings yet
- Recruitment Process Outsourcing PDFDocument4 pagesRecruitment Process Outsourcing PDFDevesh NamdeoNo ratings yet
- PC2000-8 Spec SheetDocument20 pagesPC2000-8 Spec SheetNeeraj ChauhanNo ratings yet
- Resume LittletonDocument1 pageResume Littletonapi-309466005No ratings yet
- House Staff OrderDocument2 pagesHouse Staff OrderTarikNo ratings yet
- 04 DosimetryDocument104 pages04 DosimetryEdmond ChiangNo ratings yet
- Bulletin - February 12, 2012Document14 pagesBulletin - February 12, 2012ppranckeNo ratings yet
- Chrysler Dodge Ram Jeep Drive Cycle InformationDocument2 pagesChrysler Dodge Ram Jeep Drive Cycle InformationslpkthNo ratings yet
- Bagi CHAPT 7 TUGAS INGGRIS W - YAHIEN PUTRIDocument4 pagesBagi CHAPT 7 TUGAS INGGRIS W - YAHIEN PUTRIYahien PutriNo ratings yet
- Electrostatics Practice ProblemsDocument4 pagesElectrostatics Practice ProblemsMohammed Aftab AhmedNo ratings yet
- Module 11 Activity Based CostingDocument13 pagesModule 11 Activity Based CostingMarjorie NepomucenoNo ratings yet
- Only Great Minds Can Read This Based On Cambridge University StudyDocument7 pagesOnly Great Minds Can Read This Based On Cambridge University StudyabotNo ratings yet
- REM630 Broch 756825 LRENdDocument6 pagesREM630 Broch 756825 LRENdsihamuNo ratings yet
- Bo Sanchez-Turtle Always Wins Bo SanchezDocument31 pagesBo Sanchez-Turtle Always Wins Bo SanchezCristy Louela Pagapular88% (8)
- Lesson Plan - Sight Word ObservationDocument2 pagesLesson Plan - Sight Word Observationapi-253277023No ratings yet
- Yazaki BrochureDocument4 pagesYazaki Brochureguzman_10No ratings yet
- Bachelors of Engineering: Action Research Project - 1Document18 pagesBachelors of Engineering: Action Research Project - 1manasi rathiNo ratings yet
- Ielts Reading Actual Tests With Suggested Answers Oct 2021 JDocument508 pagesIelts Reading Actual Tests With Suggested Answers Oct 2021 JHarpreet Singh JohalNo ratings yet
- Coastal Blue Carbon - Methods For Assessing Carbon Stocks and Emissions Factors in Mangroves Tidal Salt Marshes and Seagrass MeadowsDocument182 pagesCoastal Blue Carbon - Methods For Assessing Carbon Stocks and Emissions Factors in Mangroves Tidal Salt Marshes and Seagrass Meadowsapi-245803001No ratings yet
- LAB Find Out The Bottle ContentsDocument4 pagesLAB Find Out The Bottle ContentschanNo ratings yet
- Pemisah ZirconDocument10 pagesPemisah ZirconLorie Banka100% (1)
- History of The Hadith, Dr. Muhammad HameedullahDocument0 pagesHistory of The Hadith, Dr. Muhammad HameedullahAMEEN AKBAR100% (4)
- Solutions For Tutorial Exercises Association Rule Mining.: Exercise 1. AprioriDocument5 pagesSolutions For Tutorial Exercises Association Rule Mining.: Exercise 1. AprioriMarkib Singh AdawitahkNo ratings yet
- Auditing BasicsDocument197 pagesAuditing BasicsMajanja AsheryNo ratings yet
- BIOL 2300 Homework 2 Summer2019Document2 pagesBIOL 2300 Homework 2 Summer2019Tanner JohnsonNo ratings yet
- A Technical Report ON Centre of Pressure ONA Plane Surface ExperimentDocument13 pagesA Technical Report ON Centre of Pressure ONA Plane Surface ExperimentVictor OwolekeNo ratings yet
- Test Bank For Body Structures and Functions 11th Edition Ann ScottDocument27 pagesTest Bank For Body Structures and Functions 11th Edition Ann Scottpellucidutter.uka6lr100% (38)
- Unit 12 BriefDocument7 pagesUnit 12 Briefapi-477397447No ratings yet
- State of The Art in Research On MicrogridsDocument36 pagesState of The Art in Research On MicrogridsDulal MannaNo ratings yet
- Curriculum Vitae: Career ObjectiveDocument3 pagesCurriculum Vitae: Career ObjectiveRākesh Rakhi100% (1)
- Cisco Nexus 7000 Introduction To NX-OS Lab GuideDocument38 pagesCisco Nexus 7000 Introduction To NX-OS Lab Guiderazzzzzzzzzzz100% (1)