You might also like
- Benignlesionshanisah 161129150208Document71 pagesBenignlesionshanisah 161129150208Mohammad Saadullah Khan KakarNo ratings yet
- Uterine Fibroids: By: DR Dolapo AduDocument35 pagesUterine Fibroids: By: DR Dolapo AduAdu DolapoNo ratings yet
- Theory of Myoma Uteri: Gede Nanda Surya WijayaDocument32 pagesTheory of Myoma Uteri: Gede Nanda Surya WijayaNandaSuryaWijayaNo ratings yet
- Liomyoma (Fibroid) : DR Henan DH Skheel 2016 5 Year Directed LectureDocument11 pagesLiomyoma (Fibroid) : DR Henan DH Skheel 2016 5 Year Directed LectureAnonymous UHnQSkxLBDNo ratings yet
- Chapter 4Document9 pagesChapter 4Lennie LennieNo ratings yet
- Myoma EndometrialDocument26 pagesMyoma EndometrialYulia PratiwiNo ratings yet
- Endometriosis O&g PresentationDocument31 pagesEndometriosis O&g PresentationChauthiran Agamudaiyar100% (1)
- FibroidsDocument5 pagesFibroids010527anwNo ratings yet
- Myoma NewwwDocument46 pagesMyoma NewwwNandaSuryaWijayaNo ratings yet
- Fibroids: DR F HoveDocument18 pagesFibroids: DR F HoveKelvin MaikanaNo ratings yet
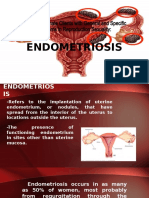
- ENDOMETRIOSISDocument29 pagesENDOMETRIOSISMaria ClaraNo ratings yet
- Benign and Malignant Tumor of UterusDocument138 pagesBenign and Malignant Tumor of UterusMuhammad HaziqNo ratings yet
- Benign Dis of The UterusDocument22 pagesBenign Dis of The UterusAsraa RashedNo ratings yet
- Fibroids PresentationDocument6 pagesFibroids Presentationapi-237061134No ratings yet
- Benign ConditionsDocument40 pagesBenign ConditionsnoreenfatimamaanNo ratings yet
- Fibroid Uterus NewDocument98 pagesFibroid Uterus NewBi PinNo ratings yet
- Uterine Fibroids Are NoncancerousDocument3 pagesUterine Fibroids Are NoncancerousNeha BhasinNo ratings yet
- Gynecologic Disorders 2Document2 pagesGynecologic Disorders 2LAXA FRANCINENo ratings yet
- Sakila MurmuDocument47 pagesSakila MurmuSakila murmuNo ratings yet
- Non-Neoplastic Disorders of Breast: Dr. Naw May Emerald Faculty of Medicine & Health Sciences UCSI UniversityDocument45 pagesNon-Neoplastic Disorders of Breast: Dr. Naw May Emerald Faculty of Medicine & Health Sciences UCSI UniversitySindhu BabuNo ratings yet
- Uterine FibroidsDocument46 pagesUterine FibroidsRavindranatha AnNo ratings yet
- Uterine FibroidDocument6 pagesUterine FibroidrenjithNo ratings yet
- Ovarian Cyst As GroupDocument54 pagesOvarian Cyst As GroupZaynab Abdul WahidNo ratings yet
- Female Reproductive - 3, Dub, Uterus Lesions, Turner SyndromeDocument34 pagesFemale Reproductive - 3, Dub, Uterus Lesions, Turner Syndromeindu mathiNo ratings yet
- Fibroid UterusDocument12 pagesFibroid Uterusvincentsharon100% (3)
- Tumor Payudara: I Made Andre PradnyanaDocument38 pagesTumor Payudara: I Made Andre PradnyanaAndre PradnyanaNo ratings yet
- UterinemyomasDocument1 pageUterinemyomasRian LaborNo ratings yet
- Fibroid Uterus 2019Document60 pagesFibroid Uterus 2019Mahmoud Abu Al AmrainNo ratings yet
- Myoma Utrei: Gynecology DepartmentDocument33 pagesMyoma Utrei: Gynecology DepartmentD.A.B.MNo ratings yet
- Fibroids by EasterDocument7 pagesFibroids by EasterIGA ABRAHAMNo ratings yet
- EndometriosisDocument50 pagesEndometriosisHannah Eloise MagsinoNo ratings yet
- Myoma of The UterusDocument22 pagesMyoma of The UterusSemon YohannesNo ratings yet
- Uterine Fibroid-IzzatDocument20 pagesUterine Fibroid-IzzatcopperNo ratings yet
- Benign Breast Disorders: Diani KartiniDocument27 pagesBenign Breast Disorders: Diani KartiniAngga ArioNo ratings yet
- Uterine FibroidsDocument47 pagesUterine FibroidsMoh Aldhy HusaintNo ratings yet
- Myoma Uteri: Pregnancy PubertyDocument9 pagesMyoma Uteri: Pregnancy PubertyJaja RamosNo ratings yet
- Abnormal Uterine BleedingDocument31 pagesAbnormal Uterine Bleedingnancy voraNo ratings yet
- Fibroids Miracle Cure: The Ultimate Fibroids Diet To Heal NaturallyFrom EverandFibroids Miracle Cure: The Ultimate Fibroids Diet To Heal NaturallyRating: 3.5 out of 5 stars3.5/5 (7)
- Fibroids 102307Document44 pagesFibroids 102307bazuu mbwegzeNo ratings yet
- MSN Ii An-Uterine FibroidDocument33 pagesMSN Ii An-Uterine FibroidSifanaNo ratings yet
- Also Called Uterine Leiomyoma, Myoma, Myomata Uteri, FibromyomaDocument25 pagesAlso Called Uterine Leiomyoma, Myoma, Myomata Uteri, Fibromyomashygirl72No ratings yet
- Breast CancerDocument69 pagesBreast CancerRayanNo ratings yet
- Ultrasound Breast ScanningDocument36 pagesUltrasound Breast ScanningPhuntsho Ongmo100% (1)
- 9 MyomaDocument36 pages9 MyomaDawit g/kidanNo ratings yet
- Fibroid Uterus: 3. SubmucousDocument3 pagesFibroid Uterus: 3. SubmucousSuhas IngaleNo ratings yet
- ENDOMETRIOSISDocument13 pagesENDOMETRIOSISAngel SaraNo ratings yet
- Uterine FibroidDocument46 pagesUterine FibroidAfiqi FikriNo ratings yet
- Gynaecological Diseases in PregnancyDocument76 pagesGynaecological Diseases in PregnancyKarishma Shroff67% (9)
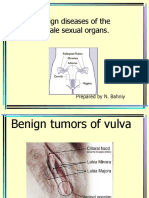
- Benign Diseases of The Female Sexual Organs.: Prepared by N. BahniyDocument32 pagesBenign Diseases of The Female Sexual Organs.: Prepared by N. BahniyDianne ObiNo ratings yet
- Uterine FibroidsDocument25 pagesUterine FibroidsMarie Eulie PatinoNo ratings yet
- Natural History AND Classification FibroidDocument8 pagesNatural History AND Classification FibroidRajhmuniran KandasamyNo ratings yet
- Breast Disorders: Wirsma Arif Harahap Surgical Oncologist Surgery DepartmentDocument82 pagesBreast Disorders: Wirsma Arif Harahap Surgical Oncologist Surgery DepartmentMetha Arsilita HulmaNo ratings yet
- 4.. ReproDocument61 pages4.. Reprosabin luitelNo ratings yet
- Fibriod: Women Barrier To Pregnancy Brief Discription of Fibriod and How It DevelopsDocument10 pagesFibriod: Women Barrier To Pregnancy Brief Discription of Fibriod and How It DevelopsRahil ShaikhNo ratings yet
- Endometrial PolypsDocument14 pagesEndometrial PolypsMusaNo ratings yet
- Benign Breast Diseases - Santhosh.SDocument18 pagesBenign Breast Diseases - Santhosh.SSandy KingNo ratings yet
- Effects of Aging in Endocrine SystemDocument5 pagesEffects of Aging in Endocrine Systemapi-3718174No ratings yet
- Benign Disorders and Diseases of The BreastDocument44 pagesBenign Disorders and Diseases of The BreastRoy Acosta GumbanNo ratings yet
- Uterine Fibroids & EndometriosisDocument82 pagesUterine Fibroids & EndometriosisDuncan Jackson67% (3)
- Premalignant Lesions of The Uterine Cervix - Sundhed - DKDocument7 pagesPremalignant Lesions of The Uterine Cervix - Sundhed - DKPavel BerlinschiNo ratings yet
- Pelvic Pain - Sundhed - DKDocument11 pagesPelvic Pain - Sundhed - DKPavel BerlinschiNo ratings yet
- Differential Diagnosis of Common Gynecological Complaints - Sundhed - DKDocument7 pagesDifferential Diagnosis of Common Gynecological Complaints - Sundhed - DKPavel BerlinschiNo ratings yet
- Intrapartum Ultrasonography For Labor ManagementDocument198 pagesIntrapartum Ultrasonography For Labor ManagementPavel BerlinschiNo ratings yet
- Polycystic Ovary Syndrome (PCOS) - Reproductive and Metabolic Aspects - Sundhed - DKDocument8 pagesPolycystic Ovary Syndrome (PCOS) - Reproductive and Metabolic Aspects - Sundhed - DKPavel BerlinschiNo ratings yet
- Stages of Puberty - Sundhed - DKDocument6 pagesStages of Puberty - Sundhed - DKPavel BerlinschiNo ratings yet
- Benign Pelvic Tumors - Sundhed - DKDocument6 pagesBenign Pelvic Tumors - Sundhed - DKPavel BerlinschiNo ratings yet
- Escala de Compulsividad SexualDocument16 pagesEscala de Compulsividad SexualCristina GarcíaNo ratings yet
- Personal Record Form CompleteDocument5 pagesPersonal Record Form CompleteFrank BloomfieldNo ratings yet
- Project On Amount of Caffeine in Tea LeavesDocument10 pagesProject On Amount of Caffeine in Tea LeaveslllNo ratings yet
- Joining Instructions Indian Military Academy (IMA) Dehradun - 28-Nov-2011 - IMAJOININGINSTRUCTIONSDocument29 pagesJoining Instructions Indian Military Academy (IMA) Dehradun - 28-Nov-2011 - IMAJOININGINSTRUCTIONSChander JoonNo ratings yet
- Patho SlidesDocument79 pagesPatho SlidesFYMNo ratings yet
- Laboratory Evaluation of PlateletsDocument4 pagesLaboratory Evaluation of Plateletscherry nokiaNo ratings yet
- Cervical Cancer Differential DiagnosesDocument8 pagesCervical Cancer Differential DiagnosesDebi SumarliNo ratings yet
- Wa0013.Document15 pagesWa0013.Simonia CoutinhoNo ratings yet
- Endodontic TT OutcomesDocument22 pagesEndodontic TT OutcomesritikaNo ratings yet
- Renr Week 7th 2017 Questions SheetDocument21 pagesRenr Week 7th 2017 Questions SheetSasha UterNo ratings yet
- OB Nursing Bullets PNLEDocument25 pagesOB Nursing Bullets PNLEACNo ratings yet
- HessDocument18 pagesHessKeith Nester Arines Lavin100% (1)
- Nursing Care Plan Drug Study Pudw - BalaDocument5 pagesNursing Care Plan Drug Study Pudw - BalaSolsona Natl HS MaanantengNo ratings yet
- Structure of Chemical Componds ImpuritiesDocument6 pagesStructure of Chemical Componds ImpuritiesJorge Oswaldo Toro Jaimes100% (1)
- E-Book Seminar PAPDI Kota Bekasi skp8Document5 pagesE-Book Seminar PAPDI Kota Bekasi skp8Miftah Nur AndamsariNo ratings yet
- 2014 ImatDocument25 pages2014 ImatNoorNo ratings yet
- Exotic Companion Medicine HandbookDocument585 pagesExotic Companion Medicine HandbookJera Berkana75% (4)
- HYPERTENSION-WPS OfficeDocument4 pagesHYPERTENSION-WPS OfficeAMOS MELINo ratings yet
- Mental Health in IndiaDocument6 pagesMental Health in IndiaStarlin MythriNo ratings yet
- Forest Monasteries Sri LankaDocument21 pagesForest Monasteries Sri LankakdkdkNo ratings yet
- Ajeph Id45Document6 pagesAjeph Id45noneofyabiznasNo ratings yet
- Approach To Patient With Diseases of The Kidney and Urinary Tract FINALDocument9 pagesApproach To Patient With Diseases of The Kidney and Urinary Tract FINALgelskNo ratings yet
- Neonatal Care Protocol For Hospital PhysiciansDocument648 pagesNeonatal Care Protocol For Hospital PhysiciansИван Мельник100% (2)
- SMLE 13 - MedicalDocument850 pagesSMLE 13 - MedicalSumayyia QamarNo ratings yet
- (Michael G. Newman, Henry Takei, Perry R. KlokkevoDocument5,032 pages(Michael G. Newman, Henry Takei, Perry R. KlokkevoDoris OteroNo ratings yet
- ps52 2015 Guidelines For Transport of Critically Ill Patients PDFDocument12 pagesps52 2015 Guidelines For Transport of Critically Ill Patients PDFPalwasha MalikNo ratings yet
- Peh 4 Module 3Document134 pagesPeh 4 Module 3burner accNo ratings yet
- Treatment Strategies For Methicillin-ResistantDocument12 pagesTreatment Strategies For Methicillin-ResistantSolRamirezNo ratings yet
- Guidelines For Management of Endometrial CarcinomaDocument41 pagesGuidelines For Management of Endometrial CarcinomaVeenaNo ratings yet
- Patrick Callaghan, Helen Waldock-Emergencies in Mental Health Nursing-Oxford University Press (2013)Document195 pagesPatrick Callaghan, Helen Waldock-Emergencies in Mental Health Nursing-Oxford University Press (2013)VidákZsigmond100% (2)