You might also like
- Casual Sex AgreementDocument5 pagesCasual Sex Agreementpingavin84% (19)
- RoughdraftlimbaughessayDocument5 pagesRoughdraftlimbaughessayapi-253782349No ratings yet
- How To Implement Sex Education Effectively in Sri Lanka PDFDocument7 pagesHow To Implement Sex Education Effectively in Sri Lanka PDFsachintyarajapakse0% (1)
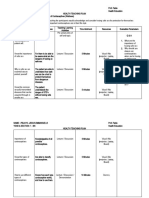
- Teaching PlanDocument6 pagesTeaching PlanE.J. PelayoNo ratings yet
- DOH ProgramsDocument114 pagesDOH ProgramsAlyssandra Luceno100% (6)
- Nigeria: National Policy On HIV/AIDSDocument65 pagesNigeria: National Policy On HIV/AIDSState House NigeriaNo ratings yet
- Unit 3Document39 pagesUnit 3vikas singhNo ratings yet
- C11 P07 National Aids Control ProgrammeDocument32 pagesC11 P07 National Aids Control ProgrammeChandana KrishnaNo ratings yet
- National Aids Control ProgrammeDocument3 pagesNational Aids Control Programmearunjv1234No ratings yet
- National AIDS Control ProgramDocument29 pagesNational AIDS Control ProgramMonalisha SinghNo ratings yet
- DOC-20240227-WA0005_##document##Document15 pagesDOC-20240227-WA0005_##document##vinushakaveripakam26No ratings yet
- India's National AIDS Control Programme (NACPDocument7 pagesIndia's National AIDS Control Programme (NACPViswa GiriNo ratings yet
- Seminar On: National AIDS Control Programme: Subject: Community Health Nursing IIDocument22 pagesSeminar On: National AIDS Control Programme: Subject: Community Health Nursing IIAkriti SharmaNo ratings yet
- GESI - From NACO - CleanDocument35 pagesGESI - From NACO - CleanMatin Ahmad KhanNo ratings yet
- DR - Basavaraj.S.Bagli P.G.Scholar Batch 2009-10 Dept of TST, NIUM BangaloreDocument36 pagesDR - Basavaraj.S.Bagli P.G.Scholar Batch 2009-10 Dept of TST, NIUM BangaloreRaj BagliNo ratings yet
- National Aids Control ProgDocument45 pagesNational Aids Control ProgGirishkumar KrishnaNo ratings yet
- 28) Hiv, Sti & TBDocument101 pages28) Hiv, Sti & TBHasabo AwadNo ratings yet
- ASSIGNMENT ON HIV ProgrammeDocument29 pagesASSIGNMENT ON HIV ProgrammeSuman MondalNo ratings yet
- 14.6aids Control ProgrammeDocument9 pages14.6aids Control Programmevenkat krishnanNo ratings yet
- Control STDs with RTI ProgrammeDocument33 pagesControl STDs with RTI Programmeayushi rainaNo ratings yet
- Condom Promotion: National AIDS Control Programme, Phase-III, IndiaDocument26 pagesCondom Promotion: National AIDS Control Programme, Phase-III, IndiaSneha SawantNo ratings yet
- National Aids Control Programmes: DR Shaila Parveen Associate Professor Dept of Social Work M.G.Kashi Vidyapith VaranasiDocument17 pagesNational Aids Control Programmes: DR Shaila Parveen Associate Professor Dept of Social Work M.G.Kashi Vidyapith VaranasiUday MajumderNo ratings yet
- Utures Roup Urope: Service AreasDocument2 pagesUtures Roup Urope: Service AreasFuturesGroup1No ratings yet
- Seminar on National Health and Population PoliciesDocument39 pagesSeminar on National Health and Population Policiesshubham rathodNo ratings yet
- Annex I National Leprosy Eradication ProgrammeDocument5 pagesAnnex I National Leprosy Eradication ProgrammespmdocNo ratings yet
- National Health ProgramsDocument19 pagesNational Health ProgramsSANANo ratings yet
- NSP 4th 2018-2022 - Draft-250517-2Document61 pagesNSP 4th 2018-2022 - Draft-250517-2Mohiuddin AhmedNo ratings yet
- PEPFAR SG Application 2017final3Document17 pagesPEPFAR SG Application 2017final3miadjafar463No ratings yet
- Achieving Universal Health CoverageDocument37 pagesAchieving Universal Health CoveragemariamNo ratings yet
- National Aids Control ProgrammeDocument77 pagesNational Aids Control Programmeangayarkanni100% (3)
- NCDs ControlDocument10 pagesNCDs ControlRam Bhushan DasNo ratings yet
- Health Planning AssignmentDocument7 pagesHealth Planning AssignmentShailjaVajpaiNo ratings yet
- HIV Prevention Module StrategiesDocument12 pagesHIV Prevention Module StrategieslebogangNo ratings yet
- Measles InitiativeDocument29 pagesMeasles InitiativeachintbtNo ratings yet
- National Health Programmes in IndiaDocument8 pagesNational Health Programmes in IndiaRohit SharmaNo ratings yet
- Module II, Gender and HIV AIDS Mainstreaming - For DAs - NZTDocument17 pagesModule II, Gender and HIV AIDS Mainstreaming - For DAs - NZTDDE1964No ratings yet
- Health Programs in India - RNTCPDocument28 pagesHealth Programs in India - RNTCPAkash Mittal100% (1)
- DRC Economic Contributions and WHO's RoleDocument20 pagesDRC Economic Contributions and WHO's RoleEurich EstradaNo ratings yet
- National Minimum Prevention MPPI GuideDocument20 pagesNational Minimum Prevention MPPI GuideEmmanuel Umo EffiongNo ratings yet
- Breaking The BarriersDocument36 pagesBreaking The BarriersKaramchedu Vignani VijayagopalNo ratings yet
- Clinical Mentorship in Public Health SettingsDocument58 pagesClinical Mentorship in Public Health Settingshappyraam0% (1)
- Modelos de Transmisión VIH BelizeDocument85 pagesModelos de Transmisión VIH BelizeDennis ValvertNo ratings yet
- Hes 409, Week 1-3Document9 pagesHes 409, Week 1-3sodiqajayi2018No ratings yet
- Newer AntifungalsDocument67 pagesNewer AntifungalsElga MuralidharanNo ratings yet
- 4058 99135 MakurdiDocument111 pages4058 99135 MakurdiSunkanmi FadojuNo ratings yet
- Final Info KitDocument42 pagesFinal Info KitDolly BenitezNo ratings yet
- PrEP-Training Slides For ProvidersDocument149 pagesPrEP-Training Slides For ProvidersGETNET TESEMANo ratings yet
- This Document Contains Text Automatically Extracted From A PDF or Image File. Formatting May Have Been Lost and Not All Text May Have Been RecognizedDocument23 pagesThis Document Contains Text Automatically Extracted From A PDF or Image File. Formatting May Have Been Lost and Not All Text May Have Been Recognizedujangketul62No ratings yet
- National AIDS Control Programme Phase-IV: Current Status and Critical AppraisalDocument71 pagesNational AIDS Control Programme Phase-IV: Current Status and Critical AppraisalNeethu Vincent100% (1)
- HIV/AIDS and STI Epidemic in NepalDocument13 pagesHIV/AIDS and STI Epidemic in Nepalsunita gurungNo ratings yet
- National Leprosy Eradication ProgrammeDocument14 pagesNational Leprosy Eradication ProgrammeAdithya AjayNo ratings yet
- Zimbabwe National HIV AIDS Strategic 2011 2015 PlanDocument69 pagesZimbabwe National HIV AIDS Strategic 2011 2015 PlanesawunyamaNo ratings yet
- National AIDS Control Program: Dr. Kanupriya ChaturvediDocument42 pagesNational AIDS Control Program: Dr. Kanupriya ChaturvedifahimalikNo ratings yet
- Primary Health CareDocument20 pagesPrimary Health CareofficialmidasNo ratings yet
- Combination HIV Prevention: Tailoring Programs To Stop TransmissionDocument2 pagesCombination HIV Prevention: Tailoring Programs To Stop TransmissionFuturesGroup1No ratings yet
- Assignment On Designing A Communication Campaign For Mexico About HIVDocument11 pagesAssignment On Designing A Communication Campaign For Mexico About HIVxhuvo50% (2)
- Planning HivDocument331 pagesPlanning HivCridoc DocumentationNo ratings yet
- National Leprosy Eradication ProgrammeDocument9 pagesNational Leprosy Eradication ProgrammeRekha ChaudharyNo ratings yet
- Learning Task 2 - An EvaluationDocument4 pagesLearning Task 2 - An EvaluationAyeng MonterdeNo ratings yet
- Assignment For National T.B ProgramDocument14 pagesAssignment For National T.B Programhaitham thabetNo ratings yet
- Issues in The ImplementationDocument10 pagesIssues in The Implementationallyza.villahermosaNo ratings yet
- Policy To Action FrameworkDocument2 pagesPolicy To Action FrameworkFuturesGroup1No ratings yet
- Aids Control Unit, Office of The President, Ministry of State For Provincial Administration and Internal SecurityDocument37 pagesAids Control Unit, Office of The President, Ministry of State For Provincial Administration and Internal SecurityfredkasomiNo ratings yet
- HIV and AIDS in The WorkplaceDocument52 pagesHIV and AIDS in The Workplacepschileshe9472No ratings yet
- HIV/AIDS Awareness: World AIDS Day (Dec 1stDocument31 pagesHIV/AIDS Awareness: World AIDS Day (Dec 1stRatneshNo ratings yet
- RM 4 GMPH W2Document15 pagesRM 4 GMPH W2Aklile ShewameneNo ratings yet
- Transformations Women Gender and Psychology 3rd Edition Crawford Test BankDocument14 pagesTransformations Women Gender and Psychology 3rd Edition Crawford Test Bankmatthewelmerwjxqf100% (20)
- SIECCAN - Q A Sexual Health Education in The Schools PDFDocument21 pagesSIECCAN - Q A Sexual Health Education in The Schools PDFNurl AinaNo ratings yet
- AbstinenceDocument32 pagesAbstinencerahul910No ratings yet
- Epidemiological Triad of HIV/AIDS: AgentDocument8 pagesEpidemiological Triad of HIV/AIDS: AgentRakib HossainNo ratings yet
- Unprotected SexDocument10 pagesUnprotected Sexapi-308820858No ratings yet
- Mycoplasma GenitaliumDocument2 pagesMycoplasma Genitaliumanurag shrivastavaNo ratings yet
- HIV Nurses Manual 2011Document273 pagesHIV Nurses Manual 2011Rahul Saha100% (1)
- Will Balbir Pasha Get AIDS FULL Case Study PDFDocument11 pagesWill Balbir Pasha Get AIDS FULL Case Study PDFSALONI GUPTANo ratings yet
- Oxford Handbook of Genitourinary Medicine HIV andDocument2 pagesOxford Handbook of Genitourinary Medicine HIV andUci AmrullahNo ratings yet
- Problem Statements from Nonprofit Proposals Target At-Risk YouthDocument20 pagesProblem Statements from Nonprofit Proposals Target At-Risk YouthWilliamNo ratings yet
- Social Change Campaign in IndiaDocument7 pagesSocial Change Campaign in IndiaGauri GargNo ratings yet
- YandereDocument9 pagesYanderebonkieto1100% (1)
- Psychology Internals ContentDocument23 pagesPsychology Internals ContentMohit KapseNo ratings yet
- HIV Prevention PresentationsDocument27 pagesHIV Prevention PresentationsAiman ButtNo ratings yet
- Sa CH5Document3 pagesSa CH5macrisio2002No ratings yet
- CH1 5 Integrating Sex Education in Basic Education CurriculumDocument86 pagesCH1 5 Integrating Sex Education in Basic Education CurriculumKelly Shane BernabeNo ratings yet
- Local Government HIV/AIDS BudgetDocument4 pagesLocal Government HIV/AIDS BudgetLeonard ArenasNo ratings yet
- Sexuality Re MasturbationDocument17 pagesSexuality Re MasturbationMaria AlvanouNo ratings yet
- Essentials of Life Span Development 3rd Edition Santrock Test Bank DownloadDocument34 pagesEssentials of Life Span Development 3rd Edition Santrock Test Bank Downloademmanuelmabelnjt7nn100% (25)
- Contraception Methods GuideDocument5 pagesContraception Methods GuideJemiline OlbocNo ratings yet
- PHT 112 Topic Quiz & Answers CompleteDocument25 pagesPHT 112 Topic Quiz & Answers CompletesammyNo ratings yet
- Unpacking of The Self (Physical, Material, Sexual, Spiritual, Political&Digital Self)Document74 pagesUnpacking of The Self (Physical, Material, Sexual, Spiritual, Political&Digital Self)Jhon Mary MarcellanaNo ratings yet
- ACTIVITY 3: Lifestyle Self-AssessmentDocument5 pagesACTIVITY 3: Lifestyle Self-AssessmentJohn Lloyd SuizoNo ratings yet