You might also like
- Eclampsia: Case Presentation Group ADocument56 pagesEclampsia: Case Presentation Group AArah Momo67% (3)
- Test Bank For Pharmacology and The Nursing Process 9th by LilleyDocument6 pagesTest Bank For Pharmacology and The Nursing Process 9th by LilleyJames Philhower100% (30)
- Obstetric Nursing Study GuideDocument69 pagesObstetric Nursing Study GuideValerie100% (3)
- Pharma-URO-U IncontinenceDocument27 pagesPharma-URO-U IncontinenceHussein AlhaddadNo ratings yet
- Handout Investigation and Management of Continence Issues in The RACF SettingDocument2 pagesHandout Investigation and Management of Continence Issues in The RACF SettingasmaaarNo ratings yet
- Urinary Incontinence Has Sesven TypesDocument55 pagesUrinary Incontinence Has Sesven TypesDhonat Flash100% (1)
- كوزرملا حاضو .د .م.أ لباب ةعماج/ بطلا ةيلك 2019 Urinary Incontinence. Involuntary loss of urine in sufficient amount or frequency to constituteDocument8 pagesكوزرملا حاضو .د .م.أ لباب ةعماج/ بطلا ةيلك 2019 Urinary Incontinence. Involuntary loss of urine in sufficient amount or frequency to constitutewzeer mohammedNo ratings yet
- Billet 23Document8 pagesBillet 23Doina CneagnitchiNo ratings yet
- Geriatric Urinary Incontinence & UTI CaseDocument9 pagesGeriatric Urinary Incontinence & UTI CaseStarr NewmanNo ratings yet
- Management of Common Geriatric ProblemsDocument27 pagesManagement of Common Geriatric ProblemsLourenz Bontia100% (2)
- Bowel Incontinence 160213121014Document20 pagesBowel Incontinence 160213121014lapyem thomasNo ratings yet
- Eliminasi Meliputi Informasi / Riwayat Pasien Pemeriksaan - Pola BAB, BAKDocument7 pagesEliminasi Meliputi Informasi / Riwayat Pasien Pemeriksaan - Pola BAB, BAKNareswari KenitenNo ratings yet
- FecalincontinanceDocument17 pagesFecalincontinancerabiullah.edu987No ratings yet
- Pharm Review For Hesi From JanaDocument8 pagesPharm Review For Hesi From Janacheyenne.black5205100% (1)
- Bowel IncontinenceDocument4 pagesBowel IncontinenceprashanthNo ratings yet
- Menstrual DisordersDocument47 pagesMenstrual DisordersKiranNo ratings yet
- Nausea and VomittingDocument24 pagesNausea and VomittingSiti Bellia Arafah XndNo ratings yet
- ConstipationDocument37 pagesConstipationHero StoreNo ratings yet
- Overaktifitas Kandung KemihDocument4 pagesOveraktifitas Kandung KemihSarah PerezNo ratings yet
- Background: ConstipationDocument7 pagesBackground: ConstipationErnesErlyanaSuryawijayaNo ratings yet
- Cu Task 11 Urinary ProblemsDocument5 pagesCu Task 11 Urinary ProblemsSamsung Note 9No ratings yet
- Urinary Incontinence From Harrison's IMDocument2 pagesUrinary Incontinence From Harrison's IMnashey08No ratings yet
- Reflex IncontinenceDocument3 pagesReflex IncontinenceMezab E RehmatNo ratings yet
- UBC - Bowel Management in Older AdultsDocument41 pagesUBC - Bowel Management in Older Adultsb BNo ratings yet
- Overview of Urinary Incontinence (UI) in The Long Term Care FacilityDocument81 pagesOverview of Urinary Incontinence (UI) in The Long Term Care Facilityالغزال الذهبيNo ratings yet
- UI-Pharmacothrapy Handbook 11th Edition 2021Document8 pagesUI-Pharmacothrapy Handbook 11th Edition 2021pbs4yvxjndNo ratings yet
- Fecal IncontinenceDocument5 pagesFecal IncontinenceDaniel Galindo SotomayorNo ratings yet
- Ariel Pemicu 5Document37 pagesAriel Pemicu 5yuliNo ratings yet
- IncontinenceDocument9 pagesIncontinenceHanaNo ratings yet
- Managing Urinary Tract Problem: FOCUS On The FollowingDocument11 pagesManaging Urinary Tract Problem: FOCUS On The FollowingLovely DaroleNo ratings yet
- Incontinentia Urine: HasnawatyDocument12 pagesIncontinentia Urine: HasnawatyafatspNo ratings yet
- Overactive Bladder Syndrome: Management and Treatment OptionsDocument7 pagesOveractive Bladder Syndrome: Management and Treatment OptionsS FznsNo ratings yet
- Kelainan Esophagus & GasterDocument83 pagesKelainan Esophagus & GasterajikwaNo ratings yet
- Urinary Incontinence: 2 PathophysiologyDocument8 pagesUrinary Incontinence: 2 PathophysiologyZiedTrikiNo ratings yet
- Responses To AlterationsDocument16 pagesResponses To AlterationsFerlyn BotalonNo ratings yet
- MedSurg Chapter 66 OutlineDocument7 pagesMedSurg Chapter 66 OutlineJosephine NavarroNo ratings yet
- Case Study OF Hypokalemia Periodic ParalysisDocument34 pagesCase Study OF Hypokalemia Periodic ParalysisVivian Montesena BreganzaNo ratings yet
- A Written Output Gerontology: Submitted byDocument15 pagesA Written Output Gerontology: Submitted bypetite15No ratings yet
- Quiz of Urinary IncontinenceDocument4 pagesQuiz of Urinary IncontinenceTiffanny Ocktivianie TobingNo ratings yet
- Urinary IncontinenceDocument17 pagesUrinary IncontinenceMohamed Na3eemNo ratings yet
- Geriatric Urologic Disorder: Assignment 1 Name:moubark Saad Alsubaie Id:201713512 To Dr:kashifDocument7 pagesGeriatric Urologic Disorder: Assignment 1 Name:moubark Saad Alsubaie Id:201713512 To Dr:kashifmoubarkNo ratings yet
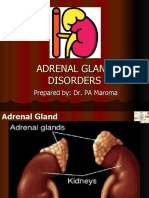
- NCMB 316 Cu14 AdrenalDocument39 pagesNCMB 316 Cu14 AdrenalJanine Dela CruzNo ratings yet
- Urinary Incontinence and Retention Grup10Document13 pagesUrinary Incontinence and Retention Grup10Deniela Jamaicy HerbertNo ratings yet
- Adrenal Disorder 1Document32 pagesAdrenal Disorder 1vanthygNo ratings yet
- OT6 - Amyotrophic Lateral SclerosisDocument19 pagesOT6 - Amyotrophic Lateral SclerosisAnnbe BarteNo ratings yet
- Urinary Incontinence: Imam D Azrul, SpuDocument20 pagesUrinary Incontinence: Imam D Azrul, SpuFarid Nurdiansyah100% (1)
- Urinary Incontinence in The Older Adult: by Kristen Cook, Pharm.D., BCPS and Linda M. Sobeski, Pharm.D., BCPSDocument18 pagesUrinary Incontinence in The Older Adult: by Kristen Cook, Pharm.D., BCPS and Linda M. Sobeski, Pharm.D., BCPSNurul HafizaNo ratings yet
- SeizuresDocument23 pagesSeizuresPooja SahuNo ratings yet
- About Urinary IncontinenceDocument6 pagesAbout Urinary IncontinenceRitesh SinghNo ratings yet
- Urinary Incontinence in Women: DR Mangala DissanayakeDocument59 pagesUrinary Incontinence in Women: DR Mangala DissanayakeAdnan WalidNo ratings yet
- Nursing Responsibilities To:: Magnesium SulfateDocument13 pagesNursing Responsibilities To:: Magnesium SulfateabrokenheartedgirlNo ratings yet
- Lecture 5 Urinary Incontinence-Part 1Document51 pagesLecture 5 Urinary Incontinence-Part 1fordsantiago01No ratings yet
- Nausea & Vomiting FINALDocument25 pagesNausea & Vomiting FINALYosr Samia Abou SediraNo ratings yet
- Urinary IncontDocument28 pagesUrinary Incontsayedmohammad mirlohiNo ratings yet
- GG Menstruasi - Dysmenorea DLLDocument35 pagesGG Menstruasi - Dysmenorea DLLPSC 119 Kota TegalNo ratings yet
- Diagnosis & Management of Urinary Incontinence: G. M. Punarbawa RSUD Prov NTB/FK UNRAMDocument39 pagesDiagnosis & Management of Urinary Incontinence: G. M. Punarbawa RSUD Prov NTB/FK UNRAMfarlamayanti100% (1)
- Hepatic FailureDocument37 pagesHepatic FailureWinston Dela FuenteNo ratings yet
- Anti-Ulcer Drug Report FinallllDocument17 pagesAnti-Ulcer Drug Report FinallllJeloume De GuzmanNo ratings yet
- Muscle RelaxantsDocument20 pagesMuscle RelaxantsJearanell LabraNo ratings yet
- Anatomy and PhysiologyDocument5 pagesAnatomy and PhysiologyAndrye Pelita ZamZam MubaroqNo ratings yet
- C H E M O T H E R A P Y: Side Effects Common Physical Side EffectsDocument7 pagesC H E M O T H E R A P Y: Side Effects Common Physical Side EffectsEuna Patricia AguilarNo ratings yet
- The Complete Guide to Chronic Constipation: Symptoms, Risks, Treatments & CuresFrom EverandThe Complete Guide to Chronic Constipation: Symptoms, Risks, Treatments & CuresNo ratings yet
- Pharma URO BPHDocument23 pagesPharma URO BPHHussein AlhaddadNo ratings yet
- Benign Prostatic Hyperplasia (BPH)Document88 pagesBenign Prostatic Hyperplasia (BPH)Hussein AlhaddadNo ratings yet
- Monobactams & CarbapenemsDocument41 pagesMonobactams & CarbapenemsHussein AlhaddadNo ratings yet
- Pharma URO MetronidazoleDocument3 pagesPharma URO MetronidazoleHussein AlhaddadNo ratings yet
- Pharma URO CephalosporinsDocument20 pagesPharma URO CephalosporinsHussein AlhaddadNo ratings yet
- Pharma URO MetronidazoleDocument3 pagesPharma URO MetronidazoleHussein AlhaddadNo ratings yet
- Anti Diare SGDocument17 pagesAnti Diare SGludoy03No ratings yet
- Opioid Adjuvant in NeuraxialDocument10 pagesOpioid Adjuvant in NeuraxialiswanlatifNo ratings yet
- Hirschsprung's Disease, PDFDocument1 pageHirschsprung's Disease, PDFMr. LNo ratings yet
- Inflammatory Myofibroblastic TumourDocument4 pagesInflammatory Myofibroblastic TumourThiruNo ratings yet
- 4 - St. Mary's - December 2020 AdmissionDocument100 pages4 - St. Mary's - December 2020 AdmissionprashantNo ratings yet
- AIA HandbookDocument3 pagesAIA HandbookahmaddanialNo ratings yet
- Pathology Review BookDocument5 pagesPathology Review BookAnas AliagaNo ratings yet
- English Task The Summery of Health Illness, Part of The Body, Medical Practicioners, Oncology and X-Ray & CT ScanDocument7 pagesEnglish Task The Summery of Health Illness, Part of The Body, Medical Practicioners, Oncology and X-Ray & CT ScanYudha HupayantiNo ratings yet
- Nursing Care of Patients With Digestive & Gastrointestinal DisordersDocument29 pagesNursing Care of Patients With Digestive & Gastrointestinal DisordersjoreyneeNo ratings yet
- Polio VaccineDocument10 pagesPolio VaccineLiiaa SiiNouunaa JupheeNo ratings yet
- 14th Century - Black DeathDocument16 pages14th Century - Black DeathJean-pierre NegreNo ratings yet
- World No-Tobacco DayDocument2 pagesWorld No-Tobacco DayAkankshaNo ratings yet
- WeBSurg Winners 42 1Document129 pagesWeBSurg Winners 42 1Ana Adam100% (1)
- Ternian HCIS InteractiveDocument10 pagesTernian HCIS InteractivetrninsgrpNo ratings yet
- Somatic RecombinationDocument5 pagesSomatic RecombinationNoor Ul NaeemNo ratings yet
- Manual of Definitive Surgical Trauma CareDocument256 pagesManual of Definitive Surgical Trauma Carebovine splendor100% (3)
- Abiraterone Acetate Plus Prednisone Versus Placebo Abiratetone LancetDocument9 pagesAbiraterone Acetate Plus Prednisone Versus Placebo Abiratetone LancetMahesh TamhaneNo ratings yet
- Canine Influenza FactsDocument5 pagesCanine Influenza FactsWIS Digital News StaffNo ratings yet
- Sodium Bicarbonate: PresentationDocument3 pagesSodium Bicarbonate: Presentationmadimadi11No ratings yet
- Nursing NotesDocument6 pagesNursing NotesTiffany SimnickNo ratings yet
- Drug StudyDocument7 pagesDrug StudyArnel MacabalitaoNo ratings yet
- Fre Orto 3Document4 pagesFre Orto 3PutriNo ratings yet
- Glass Prescription - SutrishnaDocument15 pagesGlass Prescription - SutrishnaSutrishna PramanikNo ratings yet
- What Is Caffeine? How Does Caffeine Work?Document16 pagesWhat Is Caffeine? How Does Caffeine Work?Agustinus SiswantoNo ratings yet
- Drug Study - LactuloseDocument1 pageDrug Study - LactuloseCarla Tongson MaravillaNo ratings yet
- Difference Between Serum and PlasmaDocument2 pagesDifference Between Serum and PlasmaCynthia Adeline SNo ratings yet
- Bone Tumors in Children and Adolescents-FDocument76 pagesBone Tumors in Children and Adolescents-Fkara_korumNo ratings yet
- 2016 Sep RECALLDocument49 pages2016 Sep RECALLkyahuaNo ratings yet