You might also like
- Anatomy Cheat SheetDocument3 pagesAnatomy Cheat SheetJacob100% (2)
- Methane Mitigation Global Summit Event Agenda66gJmFneLs0Uka79kaphvNEH1gLxwA14MVkznCe5Document22 pagesMethane Mitigation Global Summit Event Agenda66gJmFneLs0Uka79kaphvNEH1gLxwA14MVkznCe5Nyasimi GeoffreyNo ratings yet
- Nigeria Rice Value ChainDocument57 pagesNigeria Rice Value ChainAndres Felipe Garcia71% (7)
- Bowel IncontinenceDocument4 pagesBowel IncontinenceprashanthNo ratings yet
- ConstipationDocument40 pagesConstipationDrChhaiden PhangNo ratings yet
- NCM 116 - GIT (MODULE 5 Part II)Document6 pagesNCM 116 - GIT (MODULE 5 Part II)Meryville JacildoNo ratings yet
- Fecal Incontinence: Causes & Risk FactorsDocument2 pagesFecal Incontinence: Causes & Risk FactorsLalit KumarNo ratings yet
- Urinary IncontienceDocument102 pagesUrinary IncontienceHussein AlhaddadNo ratings yet
- Cholecystitis Viva TopicDocument4 pagesCholecystitis Viva TopicSalma NazarNo ratings yet
- Pharma-URO-U IncontinenceDocument27 pagesPharma-URO-U IncontinenceHussein AlhaddadNo ratings yet
- Kelainan Esophagus & GasterDocument83 pagesKelainan Esophagus & GasterajikwaNo ratings yet
- Overview of Urinary Incontinence (UI) in The Long Term Care FacilityDocument81 pagesOverview of Urinary Incontinence (UI) in The Long Term Care Facilityالغزال الذهبيNo ratings yet
- Garopride ManualDocument16 pagesGaropride Manualsherif_awadNo ratings yet
- Fecal IncontinenceDocument25 pagesFecal IncontinenceBinita ShresthaNo ratings yet
- CELIAC DISEASE, Hypertrophic Pyloric Stenosis, AchalasiaDocument6 pagesCELIAC DISEASE, Hypertrophic Pyloric Stenosis, Achalasiasophisticated_kim09No ratings yet
- ConstipationDocument12 pagesConstipationfrechel kimNo ratings yet
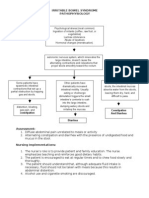
- Irritable Bowel SyndromDocument7 pagesIrritable Bowel SyndromJosni VargheseNo ratings yet
- Constipation: Done Bye: Mariam DroubiDocument13 pagesConstipation: Done Bye: Mariam DroubiFares EL DeenNo ratings yet
- Vomiting in ChildrenDocument44 pagesVomiting in ChildrenAstri Faluna SheylavontiaNo ratings yet
- Bowel ProblemsDocument6 pagesBowel ProblemsNoureen SahetoNo ratings yet
- UBC - Bowel Management in Older AdultsDocument41 pagesUBC - Bowel Management in Older Adultsb BNo ratings yet
- Irritable Bowel SyndromeDocument4 pagesIrritable Bowel Syndromedelef3No ratings yet
- Bowel EliminationDocument4 pagesBowel EliminationWarner Yague Pacariem Jr.No ratings yet
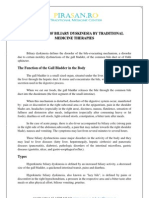
- Treatment of Biliary Dyskinesia by Traditional Medicine TherapiesDocument3 pagesTreatment of Biliary Dyskinesia by Traditional Medicine TherapiesPirasan Traditional Medicine CenterNo ratings yet
- Hirschprung DiseaseDocument10 pagesHirschprung DiseaseRichard S. RoxasNo ratings yet
- محاضرة 10Document19 pagesمحاضرة 10mkomyu088No ratings yet
- Bowel Management Following Spinal Cord InjuryDocument24 pagesBowel Management Following Spinal Cord InjuryBogdan PuscalauNo ratings yet
- ConstipationDocument37 pagesConstipationHero StoreNo ratings yet
- 4 ConstipationDocument58 pages4 ConstipationPonkiya Ankit100% (1)
- Fecal IncontinenceDocument5 pagesFecal IncontinenceDaniel Galindo SotomayorNo ratings yet
- Urinary Incontinence Has Sesven TypesDocument55 pagesUrinary Incontinence Has Sesven TypesDhonat Flash100% (1)
- Optimizing Monotherapy of Colicky Abdominal PainDocument31 pagesOptimizing Monotherapy of Colicky Abdominal PainRahmad AjahNo ratings yet
- Acute Abdomen EMDocument77 pagesAcute Abdomen EMilham santosoNo ratings yet
- Problem 2 GI - VICKA AZWITADocument65 pagesProblem 2 GI - VICKA AZWITARana RickNo ratings yet
- Ibs 2Document1 pageIbs 2Alan James Sy Cañizares100% (1)
- Nutritional Managements of Gastrointestinal Diseases/DisordersDocument54 pagesNutritional Managements of Gastrointestinal Diseases/Disordersendang sry09No ratings yet
- VomitingDocument29 pagesVomitinganusrisaranganNo ratings yet
- Functional Gastrointestinal DisordersDocument6 pagesFunctional Gastrointestinal DisordersMarwan M.No ratings yet
- Paralytic Ileus: Prepared By: Laurence A. Adena, ManDocument43 pagesParalytic Ileus: Prepared By: Laurence A. Adena, ManJanah Beado PagayNo ratings yet
- NCM 116 NB - Care of Clients With Problem in Nutrition and Gi, Metabolism and Endocrine, PerceptionDocument4 pagesNCM 116 NB - Care of Clients With Problem in Nutrition and Gi, Metabolism and Endocrine, PerceptionSureen RegularNo ratings yet
- 2300 - Module 8 - Gastrointestinal and Genitourinary EmergenciesDocument14 pages2300 - Module 8 - Gastrointestinal and Genitourinary Emergenciesmegan.abbinkNo ratings yet
- Background: ConstipationDocument7 pagesBackground: ConstipationErnesErlyanaSuryawijayaNo ratings yet
- 4 EsophagealSpasm BajaDocument6 pages4 EsophagealSpasm Bajakint manlangitNo ratings yet
- Irritable Bowel Syndrome 2Document61 pagesIrritable Bowel Syndrome 2MoonNo ratings yet
- 4 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionDocument10 pages4 NCM+116n+Lecture+Care+of+the+Clients+with+Problems+GI+Function+and+NutritionKylle AlimosaNo ratings yet
- Reflex IncontinenceDocument3 pagesReflex IncontinenceMezab E RehmatNo ratings yet
- Neurogenic BowlDocument21 pagesNeurogenic BowlFaridatul IsniyahNo ratings yet
- UI-Pharmacothrapy Handbook 11th Edition 2021Document8 pagesUI-Pharmacothrapy Handbook 11th Edition 2021pbs4yvxjndNo ratings yet
- CH 38 - Bowel EliminationDocument10 pagesCH 38 - Bowel EliminationJose GonzalezNo ratings yet
- IncontinenceDocument9 pagesIncontinenceHanaNo ratings yet
- Constipation: Ekaterine Labadze MDDocument24 pagesConstipation: Ekaterine Labadze MDsushant jainNo ratings yet
- 4 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns FinalDocument35 pages4 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns Finalevren yilmazNo ratings yet
- Fecal Incontinence: By:P. Dhilip KumarDocument8 pagesFecal Incontinence: By:P. Dhilip Kumarpreet kaurNo ratings yet
- Cu Task 11 Urinary ProblemsDocument5 pagesCu Task 11 Urinary ProblemsSamsung Note 9No ratings yet
- Motility Disorders of The GITDocument57 pagesMotility Disorders of The GITMahmoud AjinehNo ratings yet
- Quiz of Urinary IncontinenceDocument4 pagesQuiz of Urinary IncontinenceTiffanny Ocktivianie TobingNo ratings yet
- Approach To Vomiting: DR Vivek JhaDocument23 pagesApproach To Vomiting: DR Vivek JhaMukesh ThakurNo ratings yet
- Constipation and Bowel Obstructions PP Rat 10.2020Document20 pagesConstipation and Bowel Obstructions PP Rat 10.2020Vaidya M.R. PoornimaNo ratings yet
- Urinary Incontinence: Imam D Azrul, SpuDocument20 pagesUrinary Incontinence: Imam D Azrul, SpuFarid Nurdiansyah100% (1)
- Intestinal Obstructions Definition and Patient EducationDocument1 pageIntestinal Obstructions Definition and Patient EducationOlabode AdeolaNo ratings yet
- Urinary Incontinence HandoutDocument6 pagesUrinary Incontinence HandoutGautam ReddyNo ratings yet
- The Complete Guide to Chronic Constipation: Symptoms, Risks, Treatments & CuresFrom EverandThe Complete Guide to Chronic Constipation: Symptoms, Risks, Treatments & CuresNo ratings yet
- Incontinence - Management.7 ArticleDocument1 pageIncontinence - Management.7 Articlelapyem thomasNo ratings yet
- (Part 3) Acid-Base Balance-1Document7 pages(Part 3) Acid-Base Balance-1lapyem thomasNo ratings yet
- 2021 International GraduatesDocument1 page2021 International Graduateslapyem thomasNo ratings yet
- ThooeoeDocument1,142 pagesThooeoelapyem thomasNo ratings yet
- Govt. Pilot High School Rawalakot AJK Pre-Board ExamDocument2 pagesGovt. Pilot High School Rawalakot AJK Pre-Board ExamAbdul qadeerNo ratings yet
- PDF Cooling Towers Problems 1 A Cooling Tower Is Located On A Mountain Where DDDocument17 pagesPDF Cooling Towers Problems 1 A Cooling Tower Is Located On A Mountain Where DDhabboNo ratings yet
- Cetis D.D. Iso14001 Certificate 25082021 EngDocument2 pagesCetis D.D. Iso14001 Certificate 25082021 EngMonàm HadjiNo ratings yet
- CV JanetDocument2 pagesCV JanetGuar GumNo ratings yet
- Suction Strainer Boxes: Standard Specification ForDocument5 pagesSuction Strainer Boxes: Standard Specification ForKevin JosueNo ratings yet
- CD74HCT4052, CD54/74HC4053, CD54/74HC54053 High-Speed Cmos Logic Analog Multiplexers/DemultiplexersDocument34 pagesCD74HCT4052, CD54/74HC4053, CD54/74HC54053 High-Speed Cmos Logic Analog Multiplexers/DemultiplexersAndrea DispoNo ratings yet
- Boq 2020-2021 For AdnocDocument2 pagesBoq 2020-2021 For AdnocKhalid MohammedNo ratings yet
- Fairtrade ExplanationDocument2 pagesFairtrade ExplanationnabilNo ratings yet
- PMC DSR 2017-18 For Rehabilitation of BridgeDocument5 pagesPMC DSR 2017-18 For Rehabilitation of BridgeDHRUV PuneNo ratings yet
- Efficacy and Adverse Events of Oral Isotretinoin For Acne: A Systematic ReviewDocument10 pagesEfficacy and Adverse Events of Oral Isotretinoin For Acne: A Systematic ReviewFerryGoNo ratings yet
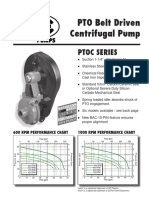
- Ptoc 03-13Document4 pagesPtoc 03-13Matias Contreras KöbrichNo ratings yet
- Lesson 09 - Gas Turbines IDocument25 pagesLesson 09 - Gas Turbines ISohaib Arshad100% (3)
- Business Vocabulary RoundDocument9 pagesBusiness Vocabulary RoundAndrei-Alexandru VasiloviciNo ratings yet
- Elementary TestDocument4 pagesElementary TestKmilo GuzmanNo ratings yet
- Korean Identity Issues Establishing Korean NationaDocument6 pagesKorean Identity Issues Establishing Korean NationaHelena AntoniukNo ratings yet
- Syllabus: Lit109: Survey of Literature This Course Does Not Require A Final ExamDocument3 pagesSyllabus: Lit109: Survey of Literature This Course Does Not Require A Final ExamJønas Søjor AlagadmøNo ratings yet
- FOMB - Letter - Senate of Puerto Rico - Response Letter Section 204 (A) (6) SB 1304 - February 7, 2024Document3 pagesFOMB - Letter - Senate of Puerto Rico - Response Letter Section 204 (A) (6) SB 1304 - February 7, 2024Metro Puerto RicoNo ratings yet
- Educational Psychology Active Learning Edition 15Th Edition Anita Woolfolk Full ChapterDocument51 pagesEducational Psychology Active Learning Edition 15Th Edition Anita Woolfolk Full Chapterdale.rolling783100% (6)
- Grilla PDFDocument8 pagesGrilla PDFLuis TestaNo ratings yet
- Zeppelin Air Manual Iphone 5 VersionDocument145 pagesZeppelin Air Manual Iphone 5 VersionTrần Nhật AnhNo ratings yet
- Yamaha Yzf r1 99 PartsDocument6 pagesYamaha Yzf r1 99 PartsRalph100% (61)
- Bajo El Hechizo: Marimba, Guitar, PianoDocument24 pagesBajo El Hechizo: Marimba, Guitar, PianoGarrison Gerard100% (1)
- Binary and Hexadecimal Number SystemDocument4 pagesBinary and Hexadecimal Number Systemkaran007_m100% (3)
- Knowledgenet - Configuring BGP On Cisco RoutersDocument0 pagesKnowledgenet - Configuring BGP On Cisco RoutersalexnemoNo ratings yet
- Product Catalogue: Atlas Copco Ground Engineering ProductsDocument40 pagesProduct Catalogue: Atlas Copco Ground Engineering ProductshamidNo ratings yet
- Gen 004 P1 ReviewerDocument6 pagesGen 004 P1 Reviewerfernandezmaekyla1330No ratings yet
- Impossible CrimeDocument2 pagesImpossible CrimeBEST OF ONE PIECENo ratings yet