You might also like
- Irritale Bowel SyndromeDocument24 pagesIrritale Bowel SyndromeUMEZURIKE DANIELNo ratings yet
- 2.6.3.7 Irritable Bowel Syndrom &kolitisDocument48 pages2.6.3.7 Irritable Bowel Syndrom &kolitisVaniNo ratings yet
- Irritable Bowel Syndrome: Heal Your Gut Naturally in 90 Days!From EverandIrritable Bowel Syndrome: Heal Your Gut Naturally in 90 Days!No ratings yet
- Unani Medicine for IBSDocument26 pagesUnani Medicine for IBSDr. Md. Shahab UddinNo ratings yet
- Problem 2 GI - VICKA AZWITADocument65 pagesProblem 2 GI - VICKA AZWITARana RickNo ratings yet
- IBS: A Guide to Irritable Bowel SyndromeDocument38 pagesIBS: A Guide to Irritable Bowel SyndromeMuhammed sherbinNo ratings yet
- Irritable Bowel SyndromeDocument22 pagesIrritable Bowel SyndromeMarium NabeelNo ratings yet
- Functional Gastrointestinal DisordersDocument6 pagesFunctional Gastrointestinal DisordersMarwan M.No ratings yet
- IBS Presentation - 1Document42 pagesIBS Presentation - 1AshishNo ratings yet
- Diare Ubaya 2Document38 pagesDiare Ubaya 2indro hariantoNo ratings yet
- Ulcerative Colitis - Crohn's DiseaseDocument68 pagesUlcerative Colitis - Crohn's DiseaseZulfan RizkyNo ratings yet
- DyspepsiaDocument4 pagesDyspepsiaaliceNo ratings yet
- IBS: Understanding Irritable Bowel SyndromeDocument17 pagesIBS: Understanding Irritable Bowel SyndromearienrachmanNo ratings yet
- Dyspepsia and Gastritis GuideDocument80 pagesDyspepsia and Gastritis GuideSoumya Ranjan PandaNo ratings yet
- NSG 306-1Document56 pagesNSG 306-1Anifowose samsonNo ratings yet
- Gerd Gerd Gerd: Dr. Rocky Danilo Willis, M.D., AMTDocument31 pagesGerd Gerd Gerd: Dr. Rocky Danilo Willis, M.D., AMTRocky Willis100% (1)
- Evaluation of GIT Dr. Bereket Molla TigabuDocument44 pagesEvaluation of GIT Dr. Bereket Molla Tigabuphoto copyhemnNo ratings yet
- Gastrointestinal SystemDocument41 pagesGastrointestinal Systemayesharajput5110No ratings yet
- Dyspepsia in Children SBDocument45 pagesDyspepsia in Children SBaira ramadhaniNo ratings yet
- GIT DisordersDocument171 pagesGIT DisordersKatrina PonceNo ratings yet
- Irritable Bowel SyndromeDocument19 pagesIrritable Bowel SyndromeOlga GoryachevaNo ratings yet
- How to Manage Dyspepsia NaturallyDocument13 pagesHow to Manage Dyspepsia NaturallyRekam Medik RS GunturNo ratings yet
- Peptic Ulcer DiseaseDocument49 pagesPeptic Ulcer DiseaseJC LumayaNo ratings yet
- Dyspepsia: Dr. Arif Nur Widodo SP - PDDocument31 pagesDyspepsia: Dr. Arif Nur Widodo SP - PDMonica Kristina HutabaratNo ratings yet
- GIT Case Study on Defecation and ConstipationDocument21 pagesGIT Case Study on Defecation and ConstipationkheluwisNo ratings yet
- Irritable bowel syndromeDocument7 pagesIrritable bowel syndromeMohd NadeemNo ratings yet
- Ibs 6Document31 pagesIbs 6Hesham IbrahimNo ratings yet
- Dyspepsia & GERDDocument65 pagesDyspepsia & GERDFatmala Haningtyas100% (1)
- Acid Peptic Disorder and GerdDocument52 pagesAcid Peptic Disorder and GerdEbuka AniNo ratings yet
- Approach To Dyspepsia: Dr. Ghalia Abu MohsenDocument60 pagesApproach To Dyspepsia: Dr. Ghalia Abu MohsenMohammedNo ratings yet
- Constipation: Ekaterine Labadze MDDocument24 pagesConstipation: Ekaterine Labadze MDsushant jainNo ratings yet
- Pengayaan Gastro 1 - KonsepDocument43 pagesPengayaan Gastro 1 - KonsepRamaNo ratings yet
- PHYSIOLOGY AND PATHOLOGY OF DEFECATIONDocument57 pagesPHYSIOLOGY AND PATHOLOGY OF DEFECATIONMonica BellyndaNo ratings yet
- Dyspepsia ManagementDocument21 pagesDyspepsia Managementladyfame100% (1)
- CELIAC DISEASE, Hypertrophic Pyloric Stenosis, AchalasiaDocument6 pagesCELIAC DISEASE, Hypertrophic Pyloric Stenosis, Achalasiasophisticated_kim09No ratings yet
- Iritable Bowel SyndromeDocument30 pagesIritable Bowel SyndromeArnella HutagalungNo ratings yet
- 30 - Funct - Dis of Dig - Syst.Document52 pages30 - Funct - Dis of Dig - Syst.alfaz lakhaniNo ratings yet
- Gi SMB - Clin MedDocument5 pagesGi SMB - Clin MedSohil PatelNo ratings yet
- IBSDocument44 pagesIBSRizky Indah SorayaNo ratings yet
- Irritable Bowel SyndromDocument7 pagesIrritable Bowel SyndromJosni VargheseNo ratings yet
- Peptic Ulcer Disease FDocument51 pagesPeptic Ulcer Disease FSharmila Laxman Dake100% (2)
- By Wisam Gatea HaniDocument32 pagesBy Wisam Gatea HanidrfatimarizNo ratings yet
- ConstipationDocument40 pagesConstipationDrChhaiden PhangNo ratings yet
- Epigastric Pain (Up Date) Masroel GontarDocument52 pagesEpigastric Pain (Up Date) Masroel GontarTaufik Akbar Faried Lubis50% (2)
- Pediatric Gastroesophageal RefluxDocument31 pagesPediatric Gastroesophageal RefluxAbdallahMousaNo ratings yet
- Ma Cristy L. Exconde, MD, FPOGSDocument62 pagesMa Cristy L. Exconde, MD, FPOGSCAROL ANN PATITICO100% (1)
- NGRAbdominalComplaints5 16 12Document102 pagesNGRAbdominalComplaints5 16 12Timothy Eduard A. SupitNo ratings yet
- PEPTIC ULCER DISEASE 2018 EdittedDocument43 pagesPEPTIC ULCER DISEASE 2018 EdittedJumbe MohamedNo ratings yet
- IBD Treatment Options for Ulcerative Colitis and Crohn's DiseaseDocument41 pagesIBD Treatment Options for Ulcerative Colitis and Crohn's DiseaseririNo ratings yet
- GitDocument28 pagesGitjjuuko josephNo ratings yet
- RTD Ard DR ErwinDocument99 pagesRTD Ard DR ErwinMuhammad Taufiq Rustam AjiNo ratings yet
- Chapter 28 Child With A Gastrointestinal ConditionDocument85 pagesChapter 28 Child With A Gastrointestinal Conditionsey_scottNo ratings yet
- DiarrheaDocument41 pagesDiarrheaRia Puji PangestutiNo ratings yet
- Irritable Bowel Syndrome-FINALDocument43 pagesIrritable Bowel Syndrome-FINALapi-3741769100% (2)
- Chronic Abdominal Pain and Headache in An Adolescent FemaleDocument18 pagesChronic Abdominal Pain and Headache in An Adolescent FemaleEmily EresumaNo ratings yet
- H.A.M. Akil Fardah Akil: "GI Disorders" Lecture in GERIATRI System, FKUHDocument14 pagesH.A.M. Akil Fardah Akil: "GI Disorders" Lecture in GERIATRI System, FKUHCutDianafitriaNo ratings yet
- Week 7 - Pediatric GI DisturbancesDocument59 pagesWeek 7 - Pediatric GI DisturbancesLeyla GalyanoNo ratings yet
- Fecal IncontinenceDocument25 pagesFecal IncontinenceBinita ShresthaNo ratings yet
- Case Study CLD 4Document12 pagesCase Study CLD 4MoonNo ratings yet
- College of Nursing, Institute of Liver and Biliary Sciences (Ilbs)Document1 pageCollege of Nursing, Institute of Liver and Biliary Sciences (Ilbs)MoonNo ratings yet
- "Acynotic Heart Disease": Seminar OnDocument40 pages"Acynotic Heart Disease": Seminar OnMoonNo ratings yet
- CVP Monitoring Procedure ChecklistDocument2 pagesCVP Monitoring Procedure ChecklistMoon100% (1)
- Nursing Care Plan for Cardiac ConditionDocument12 pagesNursing Care Plan for Cardiac ConditionMoonNo ratings yet
- Case Study CLD 2Document15 pagesCase Study CLD 2MoonNo ratings yet
- Bibliography of CLDDocument1 pageBibliography of CLDMoonNo ratings yet
- ReferenceDocument1 pageReferenceMoonNo ratings yet
- Case Study CLD 3Document18 pagesCase Study CLD 3MoonNo ratings yet
- "Guillain Barre Syndrome": Tool OnDocument6 pages"Guillain Barre Syndrome": Tool OnMoonNo ratings yet
- Case Study CLD 1Document12 pagesCase Study CLD 1MoonNo ratings yet
- Enteral Nutrition For NursingDocument34 pagesEnteral Nutrition For NursingMoonNo ratings yet
- Emergency DrugsDocument15 pagesEmergency DrugsMoonNo ratings yet
- Catheter Care and Maintenance: Ahrq Safety Program For Long-Term Care: Hais/CautiDocument14 pagesCatheter Care and Maintenance: Ahrq Safety Program For Long-Term Care: Hais/CautiMoonNo ratings yet
- Basic Communication SkillsDocument17 pagesBasic Communication SkillsAzhar Abbas100% (40)
- Basic Communication SkillsDocument17 pagesBasic Communication SkillsAzhar Abbas100% (40)
- Seminar On Health EconomicsDocument21 pagesSeminar On Health Economicsmeenabishnoi29100% (15)
- Content GastrostomyDocument5 pagesContent GastrostomyMoonNo ratings yet
- Guillain Barre Syndrome: Multiple Choice Questions ToolDocument6 pagesGuillain Barre Syndrome: Multiple Choice Questions ToolMoonNo ratings yet
- Health Economics: Ms. Ancy Chacko Iind Year M.SC Nursing Govt. College of Nursing AlappuzhaDocument101 pagesHealth Economics: Ms. Ancy Chacko Iind Year M.SC Nursing Govt. College of Nursing Alappuzhajyoti kunduNo ratings yet
- For GI DisturbanceDocument17 pagesFor GI Disturbanceraquel maniegoNo ratings yet
- Av Aids For PrintDocument1 pageAv Aids For PrintMoonNo ratings yet
- Demo Checklist Resp and CardioDocument2 pagesDemo Checklist Resp and CardioMoonNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataDocument8 pagesNursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataMoonNo ratings yet
- Content GastrostomyDocument5 pagesContent GastrostomyMoonNo ratings yet
- Demo ChecklistDocument2 pagesDemo ChecklistMoonNo ratings yet
- Nursing Care Plan for Cardiac ConditionDocument12 pagesNursing Care Plan for Cardiac ConditionMoonNo ratings yet
- Bronchial AsthmaDocument21 pagesBronchial AsthmaMoonNo ratings yet
- Care Plan On: Submitted To: Submitted byDocument38 pagesCare Plan On: Submitted To: Submitted byMoonNo ratings yet
- Using Roger's Diffusion of Innovation Theory To Implement The Healthy Schools National AccreditationDocument6 pagesUsing Roger's Diffusion of Innovation Theory To Implement The Healthy Schools National AccreditationputriNo ratings yet
- Lifting Plan ProcedureDocument4 pagesLifting Plan ProcedureNath YauNo ratings yet
- Indian School Sohar Term II Examination 2018-19 EnglishDocument4 pagesIndian School Sohar Term II Examination 2018-19 EnglishRitaNo ratings yet
- Diesel Engine Operation and DiagDocument76 pagesDiesel Engine Operation and DiagHafiezul Hassan100% (3)
- 8.1 - Production and Diagnostic Use of UltrasoundDocument3 pages8.1 - Production and Diagnostic Use of UltrasoundTakudzwa Antony MasendekeNo ratings yet
- Model Analysis: Presented By: Nikhil V Jose Dept. of OrthodonticsDocument103 pagesModel Analysis: Presented By: Nikhil V Jose Dept. of OrthodonticsDr Nikhil jose100% (1)
- Convey 1996Document8 pagesConvey 1996Moises Tinte100% (1)
- 4801-Article Text-19217-1-10-20110701Document8 pages4801-Article Text-19217-1-10-20110701David BriggsNo ratings yet
- Laser LightDocument27 pagesLaser Lightdcool3784No ratings yet
- Pds - Sunshades Instrument CoverDocument2 pagesPds - Sunshades Instrument CoverAntonio LantiguaNo ratings yet
- MA Only Notice Explains Coverage ChangeDocument2 pagesMA Only Notice Explains Coverage ChangeAnonymous Zp7kAtNo ratings yet
- Pipe Material & Dimension Standard MatrixDocument2 pagesPipe Material & Dimension Standard MatrixHemantNo ratings yet
- HANDOUT - Cell Transport Review WorksheetDocument4 pagesHANDOUT - Cell Transport Review WorksheetDenis Martinez100% (1)
- FB6100 DSCDocument132 pagesFB6100 DSCTahir FadhilNo ratings yet
- Bacnet® Fixed Function Thermostat: For Fan Coil/Heat Pump/Conventional SystemsDocument8 pagesBacnet® Fixed Function Thermostat: For Fan Coil/Heat Pump/Conventional Systemsamjadjaved033148100% (1)
- Barriers To Nurse - Patient Communication in Saudi Arabia: An Integrative ReviewDocument10 pagesBarriers To Nurse - Patient Communication in Saudi Arabia: An Integrative Reviewmark3dasaNo ratings yet
- Neurological Assessment CaseDocument13 pagesNeurological Assessment Casedrrajmptn0% (1)
- Global Leader: in Glass IonomerDocument2 pagesGlobal Leader: in Glass IonomerAnggini ZakiyahNo ratings yet
- Multi Air Engine Seminar ReportDocument23 pagesMulti Air Engine Seminar ReportVishal ChauhanNo ratings yet
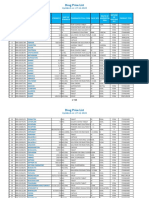
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
- Format Bahasa Inggeris UPSR 2016 ENGLISH (013) Section ADocument33 pagesFormat Bahasa Inggeris UPSR 2016 ENGLISH (013) Section AVINOTININo ratings yet
- Research 1Document7 pagesResearch 1Rhea Mae ObligarNo ratings yet
- Mandaya: Presented By: Cutad, Ray Dag-Uman, Ely Mae Cortes, MaikoDocument24 pagesMandaya: Presented By: Cutad, Ray Dag-Uman, Ely Mae Cortes, MaikoAPPLE MAE AGOSTONo ratings yet
- Power Con CorpDocument2 pagesPower Con Corpkhan4luvNo ratings yet
- RUPEX Coupling RWNDocument26 pagesRUPEX Coupling RWNWaris La Joi WakatobiNo ratings yet
- Sectors of The Indian EconomyDocument5 pagesSectors of The Indian EconomyhavejsnjNo ratings yet
- Spectralis Touch Panel Upgrade GuideDocument10 pagesSpectralis Touch Panel Upgrade GuideMohamed AbdulaalNo ratings yet
- Dezurik Balancing Valves Flow Curve 12quot 300mm 12-30-1jDocument1 pageDezurik Balancing Valves Flow Curve 12quot 300mm 12-30-1jgm_revankar3942No ratings yet
- S35MC Engine Layout and Load DiagramsDocument17 pagesS35MC Engine Layout and Load DiagramsMuhammad AlfaniNo ratings yet
- A Review of Empathy Education in NursingDocument11 pagesA Review of Empathy Education in Nursinglora ardyaNo ratings yet