You might also like
- Understanding Lymphoma: Causes, Types, Symptoms and TreatmentDocument57 pagesUnderstanding Lymphoma: Causes, Types, Symptoms and Treatmentsamar yousif mohamedNo ratings yet
- Luekemia by Dr. WongelDocument63 pagesLuekemia by Dr. Wongelmogesie1995No ratings yet
- Week 15-Mature-Lymphoid-Neoplasms-SCDocument65 pagesWeek 15-Mature-Lymphoid-Neoplasms-SCKyle CollladoNo ratings yet
- Overview of LymphomaDocument42 pagesOverview of Lymphomaadamu mohammadNo ratings yet
- LHYMPHOMADocument24 pagesLHYMPHOMACryptic LadyNo ratings yet
- Lymphoid NeoplasmsDocument52 pagesLymphoid NeoplasmsAmalia Riska GNo ratings yet
- Blockxiv Neoplasms Lymphoid 2006Document54 pagesBlockxiv Neoplasms Lymphoid 2006Ryo RyozNo ratings yet
- Acute Leukemia Types and TreatmentDocument22 pagesAcute Leukemia Types and TreatmentFelix Allen100% (1)
- Disorders of White Blood Cells and Lymphoid TissuesDocument30 pagesDisorders of White Blood Cells and Lymphoid Tissuesammar amerNo ratings yet
- Chronic Lymphoproliferative DisordersDocument108 pagesChronic Lymphoproliferative DisordersSiti NurrazanNo ratings yet
- Lymphoid Lekemia: DR Budi Enoch SPPDDocument32 pagesLymphoid Lekemia: DR Budi Enoch SPPDLia pramitaNo ratings yet
- Diseases and Tumors of Lymphoid SystemDocument97 pagesDiseases and Tumors of Lymphoid SystemamyNo ratings yet
- Lymphoma: Pro - Dr.Ahmed EisaDocument45 pagesLymphoma: Pro - Dr.Ahmed EisaOmar Mohammed100% (1)
- LymphomaDocument69 pagesLymphomaDawit g/kidanNo ratings yet
- Lymphoid Neoplasms Classification and PathologyDocument98 pagesLymphoid Neoplasms Classification and PathologyRyo RyozNo ratings yet
- Non Hodgkin Lymphoma by Dr. AnumDocument43 pagesNon Hodgkin Lymphoma by Dr. AnumHumar HaiderNo ratings yet
- Medicine Seminar Combined-1Document30 pagesMedicine Seminar Combined-1Deepanshu KumarNo ratings yet
- Chronic Lymphoid LeukaemiaDocument23 pagesChronic Lymphoid LeukaemiaAyensuaNo ratings yet
- Lymphoma Classification, Diagnosis and Treatment OverviewDocument36 pagesLymphoma Classification, Diagnosis and Treatment OverviewQasim AliNo ratings yet
- Advances in Management of NHLDocument34 pagesAdvances in Management of NHLMohammed Abd ElfattahNo ratings yet
- Non-Hodgkin'S Lymphoma: Oliveros Francis!!!!!!!!!!!!!!!!!Document48 pagesNon-Hodgkin'S Lymphoma: Oliveros Francis!!!!!!!!!!!!!!!!!francis00090No ratings yet
- Lymphoid NeoplasmsDocument39 pagesLymphoid NeoplasmsMoshe GiftNo ratings yet
- Chapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusDocument10 pagesChapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusAgnieszka WisniewskaNo ratings yet
- PATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedDocument84 pagesPATHO LEC WBC Lymph Nodes Spleen Thymus Part1 CompressedAngelo HinonNo ratings yet
- Hemopoietic SystemDocument28 pagesHemopoietic Systemyfzzhgv676No ratings yet
- LeukemiaDocument51 pagesLeukemiaKailash KhatriNo ratings yet
- Solid TumorsDocument69 pagesSolid TumorsserubimNo ratings yet
- Chronic Lymphocytic Leukemia: Dr. Tjatur Winarsanto SPPD Rs Ciremai Cirebon 2012Document17 pagesChronic Lymphocytic Leukemia: Dr. Tjatur Winarsanto SPPD Rs Ciremai Cirebon 2012Mohammad Fadel SatriansyahNo ratings yet
- Pediatric Cancers: Leukemias, Lymphomas and TreatmentDocument35 pagesPediatric Cancers: Leukemias, Lymphomas and TreatmentSarahNo ratings yet
- Chronic Myeloid LeukaemiaDocument27 pagesChronic Myeloid Leukaemiaنواف الزهرانيNo ratings yet
- Presentation (5) 2Document43 pagesPresentation (5) 2kolusam beveeNo ratings yet
- Paediatric Acute Lymphoblastic LeukemiaDocument49 pagesPaediatric Acute Lymphoblastic LeukemiaKishoreChandraKoradaNo ratings yet
- Opeyemi IdaeworDocument66 pagesOpeyemi IdaeworOpeyemi IdaeworNo ratings yet
- WBC Disorder Chap#4Document41 pagesWBC Disorder Chap#4MuhammadNo ratings yet
- Understanding Acute LeukaemiasDocument39 pagesUnderstanding Acute LeukaemiasMarvellousNo ratings yet
- LYMPH NODE CANCERDocument190 pagesLYMPH NODE CANCERNinna Isabel VictorioNo ratings yet
- 20 Lymphoid and Plasma Cell NeoplasmsDocument12 pages20 Lymphoid and Plasma Cell NeoplasmsDaphne Hernaez100% (1)
- Pathophysiology NHLDocument2 pagesPathophysiology NHLPlazer DamasenNo ratings yet
- Chronic Myeloid LeukaemiaDocument44 pagesChronic Myeloid Leukaemiaapi-273068056No ratings yet
- Malignant Lymphomas: DR Nilukshi PereraDocument48 pagesMalignant Lymphomas: DR Nilukshi PereraThaveeshaLindsayWhiteNo ratings yet
- Chronic Lymphocytic LeukemiaDocument2 pagesChronic Lymphocytic LeukemiashaguftaNo ratings yet
- L-3 Introduction To LeukemiaDocument26 pagesL-3 Introduction To LeukemiaAbood dot netNo ratings yet
- Acute Lymphoblastic LeukemiaDocument30 pagesAcute Lymphoblastic LeukemiaHarancang Kahayana0% (1)
- Lymphoma (Ean's) - 2Document29 pagesLymphoma (Ean's) - 2eanfital11No ratings yet
- Non Hodgkin'S Lymphoma: Dr. Ujjwal Chalise MD-RT Iiird Yr ResidentDocument56 pagesNon Hodgkin'S Lymphoma: Dr. Ujjwal Chalise MD-RT Iiird Yr ResidentUjjwal ChaliseNo ratings yet
- Neoplastic White Blood Cell Disorders: Leukemias, Lymphomas and MyelomaDocument45 pagesNeoplastic White Blood Cell Disorders: Leukemias, Lymphomas and MyelomayalahopaNo ratings yet
- Chronic Leukemia DR Moses KazevuDocument46 pagesChronic Leukemia DR Moses KazevuMoses Jr KazevuNo ratings yet
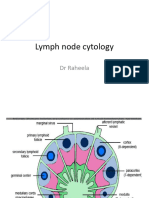
- Lymph Node CytologyDocument39 pagesLymph Node Cytologykamranghani641No ratings yet
- Lymphomas: Dr. Y.A. AdelabuDocument28 pagesLymphomas: Dr. Y.A. Adelabuadamu mohammadNo ratings yet
- Non Hodgkin LymphomaDocument9 pagesNon Hodgkin LymphomaAhmad SaifulNo ratings yet
- Malignant LymphomaDocument24 pagesMalignant LymphomaalifiaNo ratings yet
- 4th Yr GM WBC 3er and 4th Lec.Document43 pages4th Yr GM WBC 3er and 4th Lec.lanasalah.mNo ratings yet
- Chapter 13 Neoplastic Proliferations of White CellsDocument16 pagesChapter 13 Neoplastic Proliferations of White CellsOmar100% (1)
- Non-Hodgkins Lymphoma (Report)Document50 pagesNon-Hodgkins Lymphoma (Report)Dayledaniel SorvetoNo ratings yet
- Acute Myeloid LekumiaDocument34 pagesAcute Myeloid LekumiaBhuwan ThapaNo ratings yet
- LymphomasDocument34 pagesLymphomasanimesh vaidyaNo ratings yet
- Acute Lymphoblastic Leukaemia (All) : DR Y. A Kawu Mbbs/Bds Lecture 4 DEC, 2023Document36 pagesAcute Lymphoblastic Leukaemia (All) : DR Y. A Kawu Mbbs/Bds Lecture 4 DEC, 2023Muhammad Modu BulamaNo ratings yet
- Acute Myeloblastic Leukaemia: BY DR Halima Talba Consultant Haematologist Department of Haematology and BtsDocument44 pagesAcute Myeloblastic Leukaemia: BY DR Halima Talba Consultant Haematologist Department of Haematology and BtsMuhammad Modu BulamaNo ratings yet
- 11 Hematological MalignanciesDocument34 pages11 Hematological MalignanciesalitahawarbarintNo ratings yet
- Lab Session 4Document15 pagesLab Session 4Ro RyNo ratings yet
- Lab Session 2Document21 pagesLab Session 2Ro RyNo ratings yet
- Introduction To Bacteriology II - 29012024Document13 pagesIntroduction To Bacteriology II - 29012024Ro RyNo ratings yet
- Acute Lymphoblastic LeukaemiaDocument19 pagesAcute Lymphoblastic LeukaemiaRo RyNo ratings yet
- Coagulation TestingDocument29 pagesCoagulation TestingRo RyNo ratings yet
- The Monospot TestDocument9 pagesThe Monospot TestRo RyNo ratings yet
- Urine Microscopic Examination Jun2021Document2 pagesUrine Microscopic Examination Jun2021Ro RyNo ratings yet
- POLYCYTHEMIA VERA PresentationDocument12 pagesPOLYCYTHEMIA VERA PresentationRo RyNo ratings yet
- UB 2019 Guide to Undergraduate AdmissionsDocument52 pagesUB 2019 Guide to Undergraduate AdmissionsRo RyNo ratings yet
- Pharmacy: Health-SystemDocument77 pagesPharmacy: Health-Systemmalika bennadirNo ratings yet
- 2022 HRS - Aggressive B-Cell Lymphomas FINALDocument80 pages2022 HRS - Aggressive B-Cell Lymphomas FINALИван НегарэNo ratings yet
- Clasificacion de Linfomas BDocument25 pagesClasificacion de Linfomas BFiorella SalvatNo ratings yet
- Lymphoma CancerDocument34 pagesLymphoma CancerwasihaiderkNo ratings yet
- Chronic Lymphoproliferative DisordersDocument108 pagesChronic Lymphoproliferative DisordersSiti NurrazanNo ratings yet
- Mantle Patient GuidelineDocument58 pagesMantle Patient GuidelineAnonymous PrskyT0co6No ratings yet
- Blastoid Mantle Cell LymphomaDocument3 pagesBlastoid Mantle Cell LymphomaAlinaNo ratings yet
- Ask The Hematologist CompendiumDocument51 pagesAsk The Hematologist Compendiumpieterinpretoria391No ratings yet
- Ice RegimenDocument6 pagesIce RegimenNimeJi B'leaf 윤 재No ratings yet
- Onc19biopsyiso151892012 20240213 153802 0000Document18 pagesOnc19biopsyiso151892012 20240213 153802 0000asfdt.fo.sem1No ratings yet
- Mantle Cell LymphomaDocument9 pagesMantle Cell Lymphomavam buddhaNo ratings yet
- ASH Hematology Review Series - Indolent LymphomasDocument77 pagesASH Hematology Review Series - Indolent LymphomasИван НегарэNo ratings yet
- Amiloidosis JAMA 2020Document11 pagesAmiloidosis JAMA 2020Matías Jesús Flamm ZamoranoNo ratings yet
- SCD Hematological LymphomaDocument65 pagesSCD Hematological LymphomaMaria Claudia Rodriguez Zavaleta100% (1)
- B CellDocument291 pagesB CellDiana Mitrea0% (1)
- Non Hodgkin LymphomaDocument9 pagesNon Hodgkin LymphomaAhmad SaifulNo ratings yet
- A Practical Approach To Diagnosis of B-Cell Lymphomas With Diffuse LDocument8 pagesA Practical Approach To Diagnosis of B-Cell Lymphomas With Diffuse LdkbritobNo ratings yet
- About Non Hodgkin's Lymphoma (NHL) - A Quick GuideDocument6 pagesAbout Non Hodgkin's Lymphoma (NHL) - A Quick GuideDwinita ViviantiNo ratings yet