You might also like
- Chapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineDocument15 pagesChapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineandreNo ratings yet
- Gotzsche Critical Psychiatry TextbookDocument238 pagesGotzsche Critical Psychiatry Textbookronangoerl1100% (1)
- Samantha Craft's Unofficial Checklist - Females and Autism - Aspergers - The Art of AutismDocument11 pagesSamantha Craft's Unofficial Checklist - Females and Autism - Aspergers - The Art of Autismmiagiles07No ratings yet
- Attention Deficit Hyperactivity Disorder (ADHD)Document20 pagesAttention Deficit Hyperactivity Disorder (ADHD)cexaritoNo ratings yet
- Solomon SocialSkillsDocument52 pagesSolomon SocialSkillsSimona Filip100% (1)
- ADHD: Staying FocusedDocument11 pagesADHD: Staying Focusedeliron2352No ratings yet
- ADHDDocument21 pagesADHDYuniita VerayantiiNo ratings yet
- ACT Techniques 14 Interventions & Activities For Your SessionsDocument10 pagesACT Techniques 14 Interventions & Activities For Your SessionsGilang Faisal AndrianNo ratings yet
- Autism Spectrum DisorderDocument31 pagesAutism Spectrum DisorderBenson Munyan100% (1)
- Lecture 22 Attention-Deficit or Hyperactivity Disorder (ADHD)Document62 pagesLecture 22 Attention-Deficit or Hyperactivity Disorder (ADHD)jaish8904No ratings yet
- Childhood Disorders 1Document21 pagesChildhood Disorders 1Prescy Bunoan Dela CruzNo ratings yet
- Feeding and Eating DisordersDocument73 pagesFeeding and Eating DisordersMAYLENE CUENCONo ratings yet
- What Is ADHD? DSM-5 Criteria: Executive Functioning, Self-Regulation, andDocument20 pagesWhat Is ADHD? DSM-5 Criteria: Executive Functioning, Self-Regulation, andDan TomutaNo ratings yet
- Child and Adolescent Interventions: Evidence-Based Treatments For AdhdDocument22 pagesChild and Adolescent Interventions: Evidence-Based Treatments For Adhdnycsarah77No ratings yet
- Wender Utah Adult ADHD ScaleDocument3 pagesWender Utah Adult ADHD ScaleBharatNo ratings yet
- Snap DSM 5Document4 pagesSnap DSM 5Nurul PutriNo ratings yet
- Decision and Problem SolvingDocument17 pagesDecision and Problem SolvingGnaneswar PiduguNo ratings yet
- Diagnosis and Managemen T of Autistic Disorder and ADHD: Cherry Tam Supervisor: DR NG CH Ing LuenDocument47 pagesDiagnosis and Managemen T of Autistic Disorder and ADHD: Cherry Tam Supervisor: DR NG CH Ing LuenCherry TamNo ratings yet
- Disruptive Behavior of Children With Special Needs and How To Overcome Them 2. Anxiety DisordersDocument1 pageDisruptive Behavior of Children With Special Needs and How To Overcome Them 2. Anxiety DisordersPhilippe CamposanoNo ratings yet
- 606 L9 - Neurodevelopmental NOTESDocument45 pages606 L9 - Neurodevelopmental NOTESTheepekga Sivanandam100% (1)
- 1381 Westby CarolDocument70 pages1381 Westby CarolSilvia Luna OcampoNo ratings yet
- Purboyo Solek-Autism and Attention Deficit Hyperactivity Disorder (ADHD) FiDocument38 pagesPurboyo Solek-Autism and Attention Deficit Hyperactivity Disorder (ADHD) FiSupri Adi100% (2)
- Cognitive-Behavioral Therapy For Body Dysmorphic DisorderDocument9 pagesCognitive-Behavioral Therapy For Body Dysmorphic DisorderArmando ValladaresNo ratings yet
- W4-Module4 Disorders Diagnosed in Infancy, Childhood and AdolescenceDocument18 pagesW4-Module4 Disorders Diagnosed in Infancy, Childhood and AdolescenceDizon, Sharmaine L.No ratings yet
- Lecture 3 2022 - ADHD, ODD, CDDocument34 pagesLecture 3 2022 - ADHD, ODD, CDEduard DinuNo ratings yet
- ADHDDocument5 pagesADHDnikita.callistaNo ratings yet
- Attention-Deficit /hyperactivity Disorder Evaluation and Diagnosis A Practical ApproachDocument32 pagesAttention-Deficit /hyperactivity Disorder Evaluation and Diagnosis A Practical ApproachArun GeorgeNo ratings yet
- Attention-Deficit Hyperactivity DisorderDocument56 pagesAttention-Deficit Hyperactivity DisorderVikas SamotaNo ratings yet
- PPT Referat ADHD - Kevin LukitoDocument22 pagesPPT Referat ADHD - Kevin LukitonoviaNo ratings yet
- III. Disorders Diagnosed in Infancy, Childhood, and AdolescenceDocument13 pagesIII. Disorders Diagnosed in Infancy, Childhood, and AdolescenceDominic RomanillosNo ratings yet
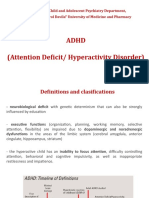
- Child and Adolescent Psychiatry Department, "Carol Davila" University of Medicine and PharmacyDocument38 pagesChild and Adolescent Psychiatry Department, "Carol Davila" University of Medicine and PharmacyAndreea BerindeaNo ratings yet
- Attention Deficit and Hyperactivity DisorderDocument11 pagesAttention Deficit and Hyperactivity DisordermengakuNo ratings yet
- Neurodevelopmental Disorders: The University of Alabama Mr. Charles WillisDocument16 pagesNeurodevelopmental Disorders: The University of Alabama Mr. Charles Willisapi-607366739No ratings yet
- Common Criteria of ADHDDocument7 pagesCommon Criteria of ADHDShahar TaorNo ratings yet
- Abnormal Psychology (Last Discussion)Document18 pagesAbnormal Psychology (Last Discussion)FLORLYN VERALNo ratings yet
- ADHD & Intellectual DisabilityDocument30 pagesADHD & Intellectual DisabilityAzkaNabilaNo ratings yet
- ADHD Guest Lecture - Child Interventions CourseDocument30 pagesADHD Guest Lecture - Child Interventions CourseOzNo ratings yet
- 16 Survivors of Violence and Trauma and Child and Adolescent PsychiatricDocument4 pages16 Survivors of Violence and Trauma and Child and Adolescent PsychiatricMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Abnormal NeurodevelopmentDocument50 pagesAbnormal NeurodevelopmentAdaugo NwauwaNo ratings yet
- Attention-Deficit ADHD Theme 2Document16 pagesAttention-Deficit ADHD Theme 2MAMA LALANo ratings yet
- Attention-Deficit/Hyperactivity Disorder (ADHD)Document38 pagesAttention-Deficit/Hyperactivity Disorder (ADHD)Amir MahmoudNo ratings yet
- Attention Deficit Hyperactivity Disorder (Adhd)Document6 pagesAttention Deficit Hyperactivity Disorder (Adhd)Sheetal PundirNo ratings yet
- Attention Deficit Hyper-Activity Disorders (ADHD) : Prepare By: Jumana AlmomaniDocument30 pagesAttention Deficit Hyper-Activity Disorders (ADHD) : Prepare By: Jumana AlmomaniJanuaryNo ratings yet
- Psych Reg Disruptive Behavioural Disorders 2009Document79 pagesPsych Reg Disruptive Behavioural Disorders 2009hopeIshanzaNo ratings yet
- AdhdDocument30 pagesAdhdНевена ЈончићNo ratings yet
- Ttention Eficit Isorder: Definitions, Epidemiology, and PathophysiologyDocument15 pagesTtention Eficit Isorder: Definitions, Epidemiology, and Pathophysiologyzhe tempNo ratings yet
- Adhd 22-6-23Document58 pagesAdhd 22-6-23ksqvrkz4dmNo ratings yet
- Types of Developmental DisordersDocument60 pagesTypes of Developmental DisordersAnshika ChaudhryNo ratings yet
- Clinical Case Analysis AdhdDocument5 pagesClinical Case Analysis AdhdSiobhan GreeneNo ratings yet
- ADHDDocument3 pagesADHDHamoud AlshehriNo ratings yet
- Behavioral DisorderDocument2 pagesBehavioral DisorderJeffrey FostanesNo ratings yet
- Childhood Psychiatric DisordersDocument16 pagesChildhood Psychiatric DisordersnonnyNo ratings yet
- Week 3Document8 pagesWeek 3Slađana MinićNo ratings yet
- 5 - ADHD Part 1Document29 pages5 - ADHD Part 1chuquer2000No ratings yet
- Attention Deficient Hyperactivity Disorders Dr. Rabia Ramadan GajumDocument24 pagesAttention Deficient Hyperactivity Disorders Dr. Rabia Ramadan GajumDr rasha FoadNo ratings yet
- Attention-Deficit: Hyperactivity DisorderDocument7 pagesAttention-Deficit: Hyperactivity DisorderMelissa CohenNo ratings yet
- The Role of Psychological Intervention To Improve Attention ADHD ChildDocument5 pagesThe Role of Psychological Intervention To Improve Attention ADHD ChildRia WindikaNo ratings yet
- Emotional DistrubanceDocument1 pageEmotional Distrubanceapi-558321133No ratings yet
- AdhdDocument28 pagesAdhdAshish SharmaNo ratings yet
- Linus-Adhd & Asd 120522Document63 pagesLinus-Adhd & Asd 120522ainzahir94No ratings yet
- PSY322 Chap 13 Neurodevelopmental and Neurocognitie DisordersDocument14 pagesPSY322 Chap 13 Neurodevelopmental and Neurocognitie DisordersGabrielle ParlaNo ratings yet
- Edu505 RevisionDocument13 pagesEdu505 RevisionStephany NyandangNo ratings yet
- Integrative Lab F2022 (Summative Assessment) 11Document7 pagesIntegrative Lab F2022 (Summative Assessment) 11Tristan WatNo ratings yet
- Attention-Deficit Hyperactivity Disorder (ADHD) : by Michael Pelster and Sarah LeggettDocument12 pagesAttention-Deficit Hyperactivity Disorder (ADHD) : by Michael Pelster and Sarah LeggettYorutsuki LuniaNo ratings yet
- Attention Deficit Hyperactivity DisorderDocument5 pagesAttention Deficit Hyperactivity DisorderTatiana ArnoldNo ratings yet
- Disruptive Behaviour DisordersDocument2 pagesDisruptive Behaviour DisordersTee Kok KeongNo ratings yet
- Specific Learning DisordersDocument33 pagesSpecific Learning DisordersGnaneswar PiduguNo ratings yet
- Autism Spectrum DisorderDocument26 pagesAutism Spectrum DisorderGnaneswar PiduguNo ratings yet
- Vanderbilt ADHDDocument7 pagesVanderbilt ADHDGnaneswar PiduguNo ratings yet
- Research Paper ReviewDocument14 pagesResearch Paper ReviewGnaneswar PiduguNo ratings yet
- For The Solution of The Caste Question, Buddha Is Not Enough, Ambedkar Is Not Enough Either, Marx Is A Must by Muppala Ranganayakamma B.R. BapujiDocument433 pagesFor The Solution of The Caste Question, Buddha Is Not Enough, Ambedkar Is Not Enough Either, Marx Is A Must by Muppala Ranganayakamma B.R. BapujiGnaneswar PiduguNo ratings yet
- CasteQuestionInIndia CPI Maoist 2021 Eng ViewDocument97 pagesCasteQuestionInIndia CPI Maoist 2021 Eng ViewGnaneswar PiduguNo ratings yet
- Strategy For Socialist RevolutionDocument10 pagesStrategy For Socialist RevolutionGnaneswar PiduguNo ratings yet
- 3 - Palmitoylethanolamide As Adjunctive Therapy For Autism Efficacy and Safety Results From A RandomDocument8 pages3 - Palmitoylethanolamide As Adjunctive Therapy For Autism Efficacy and Safety Results From A RandomEsraa SaeedNo ratings yet
- PSYC 1002M Notes Chapter 15-16Document10 pagesPSYC 1002M Notes Chapter 15-16ayd3nmcd0naldNo ratings yet
- Anti-Depressant Drugs: Facilitator Miss Ayesha BSN/RN Nursing LecturerDocument17 pagesAnti-Depressant Drugs: Facilitator Miss Ayesha BSN/RN Nursing LecturerYou TuberNo ratings yet
- Narcissist - Google SearchDocument1 pageNarcissist - Google Searchedieduardo317No ratings yet
- 8-Drugs Used in Anxiety and Panic Disprder (Edited)Document8 pages8-Drugs Used in Anxiety and Panic Disprder (Edited)himanshukumar839496No ratings yet
- Back From The Bluez - 01 - Overview of DepressionDocument9 pagesBack From The Bluez - 01 - Overview of DepressionsusanasotogarridoNo ratings yet
- Leyla - Suleymanli - Depression Among TeenagersDocument8 pagesLeyla - Suleymanli - Depression Among TeenagersLeyla SuleymanliNo ratings yet
- EPP Module 2 Assignment (Eng)Document8 pagesEPP Module 2 Assignment (Eng)anne.le6996No ratings yet
- Delirium ADocument69 pagesDelirium AAbelNo ratings yet
- Abpsy Finals ReviewerDocument9 pagesAbpsy Finals ReviewerKhaye DelgadoNo ratings yet
- Recreational TherapyDocument22 pagesRecreational TherapyKishore RathoreNo ratings yet
- Schema TherapyDocument1 pageSchema TherapyFederica ChaconNo ratings yet
- Oxford Textbook of Psychopathology Oxford Library of Psychology 4Th Edition Robert F Krueger Editor Download PDF ChapterDocument51 pagesOxford Textbook of Psychopathology Oxford Library of Psychology 4Th Edition Robert F Krueger Editor Download PDF Chapterrosie.lalonde519100% (6)
- Client Intake FormDocument4 pagesClient Intake Formzain tahirNo ratings yet
- Copy of What's in An Inkblot Some Say Not Much ArticleDocument6 pagesCopy of What's in An Inkblot Some Say Not Much ArticleNoah LoftonNo ratings yet
- Capafons Et. Al (1998)Document2 pagesCapafons Et. Al (1998)Sourav ArunNo ratings yet
- Anxiety DisordersDocument10 pagesAnxiety DisordersAhmed AntarNo ratings yet
- A Simplified Guide To Oral Antipsychotic MedicationsDocument20 pagesA Simplified Guide To Oral Antipsychotic MedicationsBruno AlencarNo ratings yet
- Nuts and Bolts of Creative Hopelessness - eBook by Russ HarrisDocument13 pagesNuts and Bolts of Creative Hopelessness - eBook by Russ HarrisTarique SaniNo ratings yet
- Bhawani THESIS - BlackDocument110 pagesBhawani THESIS - BlackAjit MishraNo ratings yet
- Brain ZapsDocument7 pagesBrain ZapsEsteban Javier Pérez MorenoNo ratings yet
- DISSOCIATIVE DISORDERS - TeachersDocument19 pagesDISSOCIATIVE DISORDERS - TeachersIano IanoNo ratings yet
- PARENT AWARENESS SEMINAR-hand OutsDocument2 pagesPARENT AWARENESS SEMINAR-hand OutsLADY ANN GRACE LAGASNo ratings yet
- Preventing RelapseDocument3 pagesPreventing RelapseGilang Faisal AndrianNo ratings yet