You might also like
- Autism Spectrum Disorders and Communication DisordersDocument12 pagesAutism Spectrum Disorders and Communication DisordersAakanksha RanjanNo ratings yet
- A level Psychology Revision: Cheeky Revision ShortcutsFrom EverandA level Psychology Revision: Cheeky Revision ShortcutsRating: 5 out of 5 stars5/5 (1)
- Neuro DevelopmentDocument11 pagesNeuro DevelopmentAmreen HameedNo ratings yet
- Emerging Trends in Autism Spectrum Disorders Diagnosis and TreatmentDocument27 pagesEmerging Trends in Autism Spectrum Disorders Diagnosis and TreatmentscribneuronNo ratings yet
- Understanding Autism Spectrum DisorderDocument24 pagesUnderstanding Autism Spectrum DisorderLove Aiza EscapalaoNo ratings yet
- Autism Spectrum Disorder: Sensory IssuesDocument4 pagesAutism Spectrum Disorder: Sensory IssuesLove Aiza EscapalaoNo ratings yet
- High-Functioning Autism Spectrum Disorder: Parent's Guide to Creating Routines, Diagnosis, Managing Sensory and Autism Awareness in Kids.From EverandHigh-Functioning Autism Spectrum Disorder: Parent's Guide to Creating Routines, Diagnosis, Managing Sensory and Autism Awareness in Kids.Rating: 5 out of 5 stars5/5 (1)
- DC0-5 TeaDocument9 pagesDC0-5 TeaJuan PabloNo ratings yet
- Autism Spectrum Disorder: Definition, Epidemiology, Etiology, Clinical Features, Diagnosis and TreatmentDocument25 pagesAutism Spectrum Disorder: Definition, Epidemiology, Etiology, Clinical Features, Diagnosis and TreatmentDrSk Samim100% (1)
- Pervasive Developmental Disorders: Dessi Aryanti Dwi Putri Gitsya Raudaful Zahira Bilingual ClassDocument39 pagesPervasive Developmental Disorders: Dessi Aryanti Dwi Putri Gitsya Raudaful Zahira Bilingual ClassCei SlametNo ratings yet
- Autism Spectrum Disorder ExplainedDocument33 pagesAutism Spectrum Disorder Explainedfcb rmaNo ratings yet
- Autism Spectrum Disorders Diagnosis and Early IdentificationDocument17 pagesAutism Spectrum Disorders Diagnosis and Early IdentificationTito100% (4)
- AutismDocument26 pagesAutismminangsung minangnengNo ratings yet
- Autism PPTDocument55 pagesAutism PPTTadesse TedlaNo ratings yet
- CASE OF AUTISM (3)Document14 pagesCASE OF AUTISM (3)Núria A.No ratings yet
- Social (Pragmatic) Communication Disorder and AutismDocument35 pagesSocial (Pragmatic) Communication Disorder and AutismHooria AmerNo ratings yet
- Understanding Special Needs ChildrenDocument32 pagesUnderstanding Special Needs Childreninvisibility checkNo ratings yet
- ASD, ADHD, DIsruptive DisorderDocument152 pagesASD, ADHD, DIsruptive DisorderRacquel Anne TanNo ratings yet
- PSYC412 Notes1Document5 pagesPSYC412 Notes1leila.belghaitNo ratings yet
- File 1663148139 0005620 AUTISMDocument45 pagesFile 1663148139 0005620 AUTISM2022824838.pasangNo ratings yet
- Review Autism Spectrum Disorders: 2000 by Cell PressDocument9 pagesReview Autism Spectrum Disorders: 2000 by Cell PressPutu Agus GrantikaNo ratings yet
- Understanding Autism Through Family PerspectivesDocument16 pagesUnderstanding Autism Through Family PerspectivesMichael BarnesNo ratings yet
- AutismDocument9 pagesAutismAmr Ramazan IbrahimNo ratings yet
- Autism AssessmentDocument37 pagesAutism AssessmentRafael Martins94% (16)
- Understanding Pervasive Developmental DisordersDocument20 pagesUnderstanding Pervasive Developmental DisordersHikari 光 Shidou100% (1)
- DSM-IV Criteria for Autism Spectrum DisordersDocument24 pagesDSM-IV Criteria for Autism Spectrum DisordersREDEEM NNo ratings yet
- Childhood Psychological DisordersDocument7 pagesChildhood Psychological DisordersineedthisforaschoolprojectNo ratings yet
- Psychiatric Disorders of Childhood PDFDocument55 pagesPsychiatric Disorders of Childhood PDFJenny Wong100% (1)
- Running Head: AUTISM 1Document14 pagesRunning Head: AUTISM 1mom2girls1boy100% (1)
- Dominica AutismDocument27 pagesDominica AutismAadeshMistryNo ratings yet
- Conduct Disorder: Dr. Jayanta Kurmi Junior Resident Dept of Psychiatry SMCHDocument50 pagesConduct Disorder: Dr. Jayanta Kurmi Junior Resident Dept of Psychiatry SMCHJayanta Kurmi100% (1)
- Austism Spectrum DisorderDocument21 pagesAustism Spectrum DisorderFrancez Anne GuanzonNo ratings yet
- Autism Spectrum Disorder: A guide with 10 key points to design the most suitable strategy for your childFrom EverandAutism Spectrum Disorder: A guide with 10 key points to design the most suitable strategy for your childNo ratings yet
- Boundless Love: Embracing The Energy And Challenges Of Special ChildrenFrom EverandBoundless Love: Embracing The Energy And Challenges Of Special ChildrenNo ratings yet
- CHAPTER 1 Thesis HiSTORICALDocument8 pagesCHAPTER 1 Thesis HiSTORICALRomae AlimaniaNo ratings yet
- A Parent's Guide to Autism Spectrum DisorderDocument15 pagesA Parent's Guide to Autism Spectrum DisordertmharishNo ratings yet
- Childhood Disorders 1. Autism: Izzy WayDocument9 pagesChildhood Disorders 1. Autism: Izzy WayKim GonzalesNo ratings yet
- Understanding Special Needs and Developmental DisordersDocument32 pagesUnderstanding Special Needs and Developmental Disordersinvisibility checkNo ratings yet
- Raising Children with Autism: 100 Things Every Parent of an Autistic Child Must KnowFrom EverandRaising Children with Autism: 100 Things Every Parent of an Autistic Child Must KnowRating: 4 out of 5 stars4/5 (4)
- Decoding Love: Navigating Dating and Relationships on the Autism SpectrumFrom EverandDecoding Love: Navigating Dating and Relationships on the Autism SpectrumNo ratings yet
- Early Intervention of Autism: A Case For Floor Time ApproachDocument28 pagesEarly Intervention of Autism: A Case For Floor Time ApproachpsicosmosNo ratings yet
- Autism Spectrum DisordersDocument26 pagesAutism Spectrum Disordersbsndbh65wcNo ratings yet
- Final Oral PSYCHOLOGYDocument10 pagesFinal Oral PSYCHOLOGYmalihah qaziNo ratings yet
- Cep 871 Case ConceptualizationDocument35 pagesCep 871 Case Conceptualizationapi-735796457No ratings yet
- Child and Adolescent DisordersDocument32 pagesChild and Adolescent Disorderscubezero100% (1)
- Summary of Dr. Anthony Attwood's The Complete Guide to Asperger's SyndromeFrom EverandSummary of Dr. Anthony Attwood's The Complete Guide to Asperger's SyndromeNo ratings yet
- Autism TalaDocument14 pagesAutism TalaAgus BarretoNo ratings yet
- Pervasive Developmental Disorders: Autisic DisorderDocument10 pagesPervasive Developmental Disorders: Autisic DisorderBinu MathewNo ratings yet
- Autism Spectrum Disorder: Fouad Tahan, M.D. PsychiatristDocument35 pagesAutism Spectrum Disorder: Fouad Tahan, M.D. PsychiatristchawkatNo ratings yet
- Persistent Impairments in Social Communication, and Restricted, Repetitive and Stereotyped Patterns If Behaviours, Interests, or ActivitiesDocument4 pagesPersistent Impairments in Social Communication, and Restricted, Repetitive and Stereotyped Patterns If Behaviours, Interests, or ActivitiesWaqas AhsanNo ratings yet
- Severe Impairments of Social Interaction PDFDocument19 pagesSevere Impairments of Social Interaction PDFjhernandez8394100% (1)
- Autism: Autism Diagnosis DSM IV MatchDocument6 pagesAutism: Autism Diagnosis DSM IV MatchReyhan VivaldyNo ratings yet
- EIU Autism 2017 HandoutDocument120 pagesEIU Autism 2017 HandoutTeofilo Palsimon Jr.No ratings yet
- Child and Adolescent PsychiatryDocument57 pagesChild and Adolescent PsychiatrySajaratul Syifaa'No ratings yet
- Specific Learning DisordersDocument33 pagesSpecific Learning DisordersGnaneswar PiduguNo ratings yet
- ADHDDocument31 pagesADHDGnaneswar PiduguNo ratings yet
- Vanderbilt ADHDDocument7 pagesVanderbilt ADHDGnaneswar PiduguNo ratings yet
- Decision and Problem SolvingDocument17 pagesDecision and Problem SolvingGnaneswar PiduguNo ratings yet
- Research Paper ReviewDocument14 pagesResearch Paper ReviewGnaneswar PiduguNo ratings yet
- Strategy For Socialist RevolutionDocument10 pagesStrategy For Socialist RevolutionGnaneswar PiduguNo ratings yet
- 5 6104878849680475329Document334 pages5 6104878849680475329ARJUN DILEEP100% (1)
- Capitalism and Mental HealthDocument4 pagesCapitalism and Mental HealthGnaneswar PiduguNo ratings yet
- CasteQuestionInIndia CPI Maoist 2021 Eng ViewDocument97 pagesCasteQuestionInIndia CPI Maoist 2021 Eng ViewGnaneswar PiduguNo ratings yet
- Proper Application of Duff Phelps ERP Adjustment PDFDocument4 pagesProper Application of Duff Phelps ERP Adjustment PDFramsiva354No ratings yet
- Trilon C Types TI enDocument11 pagesTrilon C Types TI enjuanfelipehincapieNo ratings yet
- Yoga & Diet To Prevent DepressionDocument5 pagesYoga & Diet To Prevent DepressionDietician Mrunmayee DixitNo ratings yet
- 2.factory Price - Alarm Accessories-Complete 20150325Document15 pages2.factory Price - Alarm Accessories-Complete 20150325FREE BUSINESS INTELLIGENCENo ratings yet
- 342Mass&HeatModule (3) Soln071118 OlefinPlantDocument12 pages342Mass&HeatModule (3) Soln071118 OlefinPlantmanuelNo ratings yet
- IRC Girl Shine Part 4 DigitalDocument124 pagesIRC Girl Shine Part 4 DigitalMónica SalesNo ratings yet
- Substrates P400 enDocument111 pagesSubstrates P400 enLince WijoyoNo ratings yet
- MFT28 - Greg Plitt's 4-Week Military Fitness Trainer by MET-RxDocument7 pagesMFT28 - Greg Plitt's 4-Week Military Fitness Trainer by MET-RxRayNo ratings yet
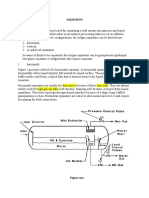
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- Appointment Letter Staff Nurse Job DescriptionDocument3 pagesAppointment Letter Staff Nurse Job DescriptionRenita ChrisNo ratings yet
- Erowid LSD (Acid) Vault - ImagesDocument2 pagesErowid LSD (Acid) Vault - ImagesAdam BruhNo ratings yet
- Music and Therapy Bun2Document17 pagesMusic and Therapy Bun2PanteaAlisaNo ratings yet
- Discontinued Tymphany LAT Products LAT500 001 PDFDocument2 pagesDiscontinued Tymphany LAT Products LAT500 001 PDFOgie FermoNo ratings yet
- Johnson Et Al.2006. Felidae PhylogenyDocument6 pagesJohnson Et Al.2006. Felidae Phylogenyaspergillus_jallNo ratings yet
- Conveying Water Distribution SEODocument90 pagesConveying Water Distribution SEOmichelghanemNo ratings yet
- Della Core DutiesDocument12 pagesDella Core DutiesSt SNo ratings yet
- Aiesha Edward Resume2Document2 pagesAiesha Edward Resume2api-491571342No ratings yet
- 03 Open Merit MBBSPrivate 2019Document149 pages03 Open Merit MBBSPrivate 2019Hasnain ZahoorNo ratings yet
- Major Emergencies in Power PlantDocument29 pagesMajor Emergencies in Power Plantsourav mahapatraNo ratings yet
- Perfect Scale Pro ManualDocument9 pagesPerfect Scale Pro ManualAnthony VargasNo ratings yet
- Rotation: Medical Intensive Care Unit (South Campus) For Interns and ResidentsDocument6 pagesRotation: Medical Intensive Care Unit (South Campus) For Interns and ResidentsHashimIdreesNo ratings yet
- Manoshe Street Takeaway MenuDocument9 pagesManoshe Street Takeaway MenuimaddakrNo ratings yet
- Uber ComplaintDocument17 pagesUber ComplaintMichael TobinNo ratings yet
- Nursing Care of The Patient Undergoing Lumbar Spinal Fusion: ReviewsDocument10 pagesNursing Care of The Patient Undergoing Lumbar Spinal Fusion: ReviewsMuammar100% (1)
- Static DischargeDocument21 pagesStatic DischargeRRNo ratings yet
- Flashcards - CP4 Preparation of A Standard Solution and Titration - Edexcel IAL Chemistry A-LevelDocument37 pagesFlashcards - CP4 Preparation of A Standard Solution and Titration - Edexcel IAL Chemistry A-LevelTravel UnlimitedNo ratings yet
- Journal Titles and DetailsDocument30 pagesJournal Titles and DetailsMinerva Medical Treatment Pvt LtdNo ratings yet
- Earth First! Climbers Guild Vol. 2Document16 pagesEarth First! Climbers Guild Vol. 2CascadiaDefenders100% (2)
- Order - Judgement Query Coram WiseDocument13 pagesOrder - Judgement Query Coram Wisesatish_CJNo ratings yet
- Effect of Non-Newtonian Fluids On The Performance of Plate Type Heat ExchangerDocument4 pagesEffect of Non-Newtonian Fluids On The Performance of Plate Type Heat Exchangerdeepika snehiNo ratings yet