You might also like
- Gynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenFrom EverandGynecology: Three Minimally Invasive Procedures You Need to Know About For: Permanent Birth Control, Heavy Menstrual Periods, Accidental Loss of Urine Plus: Modern Hormone Therapy for the Post Menopausal WomenNo ratings yet
- Group #9Document75 pagesGroup #9Dr Anais AsimNo ratings yet
- Pediatric InstrumentsDocument30 pagesPediatric InstrumentsSanjit PandeyNo ratings yet
- A Guide for the Dissection of the Dogfish (Squalus Acanthias)From EverandA Guide for the Dissection of the Dogfish (Squalus Acanthias)No ratings yet
- Mri Procedure of PNSDocument57 pagesMri Procedure of PNSAsmita BhattNo ratings yet
- A Simple Guide to the Ear and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Ear and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Mri Procedure of PNSDocument57 pagesMri Procedure of PNSAsmita BhattNo ratings yet
- IntubationDocument41 pagesIntubationNice YouNo ratings yet
- Tonsillectomy: Presented By: Nur Insyirah AbdullahDocument21 pagesTonsillectomy: Presented By: Nur Insyirah AbdullahNur InsyirahNo ratings yet
- Difficult Airway AlgorithmDocument48 pagesDifficult Airway AlgorithmshikhaNo ratings yet
- Auditory Tube and Sternocleidomastoid MuscleDocument46 pagesAuditory Tube and Sternocleidomastoid MuscleSrishti SrivastavaNo ratings yet
- Tracheostomy 8th SemesterDocument38 pagesTracheostomy 8th SemesterpotoraccosminaNo ratings yet
- Tympanoplasty: Manal Al Quaimi 207000989 2011Document39 pagesTympanoplasty: Manal Al Quaimi 207000989 2011Manal AlQuaimiNo ratings yet
- Medicine InstrumentsDocument89 pagesMedicine Instrumentsvinaynagar1994No ratings yet
- Head and Neck SurgeryDocument15 pagesHead and Neck SurgeryMedisina101100% (1)
- Presentation DH (Repaired)Document22 pagesPresentation DH (Repaired)Anmol SinghNo ratings yet
- Airway Obstruction and TracheostomyDocument44 pagesAirway Obstruction and TracheostomySindhu BabuNo ratings yet
- CholesteatomaDocument30 pagesCholesteatoma李丞永No ratings yet
- Lecture 3 Airway Management-3Document42 pagesLecture 3 Airway Management-3Bimel KottarathilNo ratings yet
- SpleenDocument69 pagesSpleenprabowoaji12No ratings yet
- Anes AirwayDocument24 pagesAnes AirwayyanaNo ratings yet
- Airway Instruments: Dr. Amr Marzouk Mohamed Assistant Lecturer of AnesthesiaDocument41 pagesAirway Instruments: Dr. Amr Marzouk Mohamed Assistant Lecturer of AnesthesiaArtha PutuNo ratings yet
- TMJ Anatomy and DisorderDocument163 pagesTMJ Anatomy and DisorderArshdeep KaurNo ratings yet
- Burst Abdomen: by DR - SuhaibDocument15 pagesBurst Abdomen: by DR - Suhaibsuhaibrehaman100% (1)
- TRACHEOSTOMTPRESENTATIONDocument37 pagesTRACHEOSTOMTPRESENTATIONStar AcademyNo ratings yet
- Open Appendicectomy: DR - Preethi G 1 Year DNB General Surgery Seven Hills Hospital VisakhapatnamDocument33 pagesOpen Appendicectomy: DR - Preethi G 1 Year DNB General Surgery Seven Hills Hospital VisakhapatnamPreethi GudipalliNo ratings yet
- Anatomy and PhysiologyDocument42 pagesAnatomy and Physiologysushma shresthaNo ratings yet
- Thyroglossal Duct CystDocument38 pagesThyroglossal Duct CystMilrose GamboaNo ratings yet
- Anesthesia in Oral SurgeryDocument41 pagesAnesthesia in Oral Surgerymed21580809No ratings yet
- Cortical Mastoid SurgeryDocument22 pagesCortical Mastoid Surgerymanu100% (1)
- Affection of Horn: Diseases of Integumentary SystemDocument31 pagesAffection of Horn: Diseases of Integumentary SystemInam khanNo ratings yet
- Indian Dental Academy: Leader in Continuing Dental EducationDocument13 pagesIndian Dental Academy: Leader in Continuing Dental Educationindian dental academyNo ratings yet
- TracheostomyDocument36 pagesTracheostomyjacnpoyNo ratings yet
- Ear AnatomyDocument107 pagesEar AnatomyalenaduisdorlfNo ratings yet
- Craniotomy FlapsDocument41 pagesCraniotomy FlapsKaramsi Gopinath NaikNo ratings yet
- (ENT SGT) Myringotomy, Myringoplasty 25.05.2023Document21 pages(ENT SGT) Myringotomy, Myringoplasty 25.05.2023Devidutta Dash 21PMB055No ratings yet
- Anatomy and Physiology of Salivary GlandsDocument71 pagesAnatomy and Physiology of Salivary GlandsArun PadikkalveetilNo ratings yet
- SplenectomyDocument69 pagesSplenectomyAgita GintingNo ratings yet
- Total Laparoscopic Hysterectomy: Andrew Doering Minimally Invasive Surgery Lab University of KentuckyDocument32 pagesTotal Laparoscopic Hysterectomy: Andrew Doering Minimally Invasive Surgery Lab University of KentuckyJunaida AfifaNo ratings yet
- Tracheostomy SlidesDocument24 pagesTracheostomy SlidesMohammed AdamNo ratings yet
- Vagina Anat, Episiotomy and MGMT of Cervical TearDocument50 pagesVagina Anat, Episiotomy and MGMT of Cervical TearCapricious BibekNo ratings yet
- 1ear AnatomyDocument33 pages1ear AnatomyMarijaNo ratings yet
- Airway ACLSDocument29 pagesAirway ACLSJoshua KosowskyNo ratings yet
- Airway ManagementDocument36 pagesAirway ManagementShobhaNo ratings yet
- Perianal Abscess - Pilonidal DiseaseDocument50 pagesPerianal Abscess - Pilonidal DiseaseAnonymous pTQIbWT2i9No ratings yet
- Tracheostomy: by Veronica Robert, MD 4 Moderator DR - SamsonDocument41 pagesTracheostomy: by Veronica Robert, MD 4 Moderator DR - SamsonMacktevin FraterinNo ratings yet
- 1-Dog Cat SpayingDocument19 pages1-Dog Cat SpayingOsama GhaziNo ratings yet
- Airwaymanagement 090810125917 Phpapp02Document41 pagesAirwaymanagement 090810125917 Phpapp02AzanReza AbdullehNo ratings yet
- Muscles of MasticationDocument112 pagesMuscles of MasticationEazhil RajNo ratings yet
- Anatomy of Nose and PNS FinalDocument125 pagesAnatomy of Nose and PNS FinalSangam AdhikariNo ratings yet
- Perineal TearsDocument44 pagesPerineal TearsMagic_OverNo ratings yet
- Inner Ear For UGDocument33 pagesInner Ear For UGdebdeepbhattacharya411No ratings yet
- Chapter 3 Airway Management in Trauma PatientDocument53 pagesChapter 3 Airway Management in Trauma PatientMGCNo ratings yet
- Airway Management: Azzam Nawab Mbbs Aanawab@imamu - Edu.saDocument48 pagesAirway Management: Azzam Nawab Mbbs Aanawab@imamu - Edu.sasamhNo ratings yet
- Tracheostomy Care: Presented by Sital B. Sharma M SC Nursing Student College of Nursing. N.B.M.C.HDocument74 pagesTracheostomy Care: Presented by Sital B. Sharma M SC Nursing Student College of Nursing. N.B.M.C.HShetal Sharma100% (1)
- 5 Eee 79626 Ca 13Document47 pages5 Eee 79626 Ca 13Aroosha JamshaidNo ratings yet
- Orchidopexy: Yuanico LiraukaDocument19 pagesOrchidopexy: Yuanico LiraukaRieza NurdinsyahNo ratings yet
- Integrated Lectures, Year III Medical Students, Gulu University Medical SchoolDocument15 pagesIntegrated Lectures, Year III Medical Students, Gulu University Medical SchoolxilcomNo ratings yet
- Chronic Trimaleolar FX DislocationDocument12 pagesChronic Trimaleolar FX DislocationIskolar MorenoNo ratings yet
- Congenital Aural AtresiaDocument34 pagesCongenital Aural Atresia李丞永No ratings yet
- Non Steroidal Anti-Inflammatory DrugsDocument2 pagesNon Steroidal Anti-Inflammatory Drugs李丞永No ratings yet
- Central Vestibular DisorderDocument37 pagesCentral Vestibular Disorder李丞永No ratings yet
- Sleep Apnea and Sleep-Disordered BreathingDocument64 pagesSleep Apnea and Sleep-Disordered Breathing李丞永No ratings yet
- How to Choose an Appropriate Anti-hypertensive DrugDocument55 pagesHow to Choose an Appropriate Anti-hypertensive Drug李丞永No ratings yet
- Salivary NeoplasmDocument29 pagesSalivary Neoplasm李丞永No ratings yet
- O To ToxicityDocument14 pagesO To Toxicity李丞永No ratings yet
- Aging and AuditoryDocument21 pagesAging and Auditory李丞永No ratings yet
- Advanced Larynx CancerDocument23 pagesAdvanced Larynx Cancer李丞永No ratings yet
- CholesteatomaDocument30 pagesCholesteatoma李丞永No ratings yet
- OflactionDocument12 pagesOflaction李丞永No ratings yet
- Peripheral Vestibular DisordersDocument42 pagesPeripheral Vestibular Disorders李丞永No ratings yet
- The Philippine Informal Reading InventoryDocument2 pagesThe Philippine Informal Reading InventoryVenilyn Cruz91% (11)
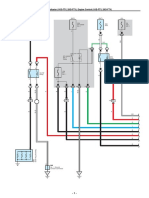
- ECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Document33 pagesECT and A/T Indicator (1KD-FTV, 2KD-FTV), Engine Control (1KD-FTV, 2KD-FTV)Erick Lizana Neyra100% (4)
- English For Military PersonnelDocument9 pagesEnglish For Military PersonnelGilang Satia LaksanaNo ratings yet
- Marketing Plan Rental LaptopDocument15 pagesMarketing Plan Rental LaptopDany AkbarNo ratings yet
- Flower Show Schedule 2015Document12 pagesFlower Show Schedule 2015api-216452145No ratings yet
- E-Katalog Warna - FullDocument43 pagesE-Katalog Warna - Fullarend alfiyantoNo ratings yet
- ACS 2000AD APPL SW Troubleshooting ManualDocument71 pagesACS 2000AD APPL SW Troubleshooting ManualFarhan Sattar0% (1)
- On Tap Giua Ky 2 MoiDocument9 pagesOn Tap Giua Ky 2 MoiPhương LêNo ratings yet
- Orca Share Media1676505355563 7031773118863093717Document42 pagesOrca Share Media1676505355563 7031773118863093717Charls Aron ReyesNo ratings yet
- Applied Soft Computing: Sandeep Singh Chauhan, Prakash KotechaDocument20 pagesApplied Soft Computing: Sandeep Singh Chauhan, Prakash KotechaCESARPINEDANo ratings yet
- Salve (Te) !: Salvete, Stephane Et Marce!Document8 pagesSalve (Te) !: Salvete, Stephane Et Marce!nicolaskelseyNo ratings yet
- 1best Practices For Migrating SAP Systems To Ora... - Oracle CommunityDocument4 pages1best Practices For Migrating SAP Systems To Ora... - Oracle CommunitymethukupallyNo ratings yet
- Ψηφιακός Γραμματισμός ΣταΟπτικοακουστικά Μέσα Σε Διαδικτυακά Περιβάλλοντα ΜάθησηςDocument19 pagesΨηφιακός Γραμματισμός ΣταΟπτικοακουστικά Μέσα Σε Διαδικτυακά Περιβάλλοντα ΜάθησηςSofos LoisosNo ratings yet
- SynopsisDocument20 pagesSynopsisMohd ShahidNo ratings yet
- ISO 261 EN 2010 - Page2 PDFDocument1 pageISO 261 EN 2010 - Page2 PDFd3bilNo ratings yet
- A Study On Impact of Social Media Marketing On Consumer BuyingDocument53 pagesA Study On Impact of Social Media Marketing On Consumer BuyingManju Mahara0% (1)
- A Modified Functionally Generated Path Technique FGP For Making Posterior Unit Metal Ceramic Crown PDFDocument8 pagesA Modified Functionally Generated Path Technique FGP For Making Posterior Unit Metal Ceramic Crown PDFDrRanjeet Kumar ChaudharyNo ratings yet
- Personal Information WorksheetDocument1 pagePersonal Information Worksheetdaniela cardonaNo ratings yet
- English Year 3 - Midterm ExaminationDocument8 pagesEnglish Year 3 - Midterm Examinationsuhaini abidinNo ratings yet
- GPSA 2nd Phase Tender For CUIS 2021-22Document1 pageGPSA 2nd Phase Tender For CUIS 2021-22Mwandembo Ushindi0% (1)
- All Bin List Check 2023Document165 pagesAll Bin List Check 2023Loise100% (3)
- Tesla - Tunguska Explosion 1908 PDFDocument9 pagesTesla - Tunguska Explosion 1908 PDFMircea Gabriel BalanNo ratings yet
- Colace (Docusate Sodium)Document1 pageColace (Docusate Sodium)E100% (1)
- Questions PetrobowlDocument58 pagesQuestions PetrobowlCuloNo ratings yet
- Lipa City Colleges Graduate SchoolDocument7 pagesLipa City Colleges Graduate SchoolRenz BrionesNo ratings yet
- Method of Statement - Pa SystemDocument15 pagesMethod of Statement - Pa SystemashifNo ratings yet
- AFST - Oct 17Document9 pagesAFST - Oct 17kimkimNo ratings yet
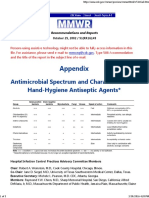
- Antimicrobial Spectrum and Characteristics of Hand-Hygiene Antiseptic AgentsDocument3 pagesAntimicrobial Spectrum and Characteristics of Hand-Hygiene Antiseptic AgentsdonsterthemonsterNo ratings yet
- On Three Monotone Approximation: Mayada Ali KareemDocument4 pagesOn Three Monotone Approximation: Mayada Ali KareemMohamed Aly SowNo ratings yet
- Analysis of The Characteristics of A Good Civil Engineer: D. Blockley and RobertsonDocument4 pagesAnalysis of The Characteristics of A Good Civil Engineer: D. Blockley and RobertsonsujupsNo ratings yet