You might also like
- Gliptins: Current Status & Future PromiseDocument46 pagesGliptins: Current Status & Future PromiseSmit ShahNo ratings yet
- Build A Borz Practical Scrap Metal Small Arms Vol9Document23 pagesBuild A Borz Practical Scrap Metal Small Arms Vol9Gia Linh Văn100% (2)
- Performance Analysis of Cooling TowerDocument7 pagesPerformance Analysis of Cooling TowerIbrahim Al-MutazNo ratings yet
- Ames Perception ExperimentsDocument108 pagesAmes Perception ExperimentsMichael RoseNo ratings yet
- ACP Insulin SlideCAST 222Document197 pagesACP Insulin SlideCAST 222charanmann9165No ratings yet
- B757-200 MPDDocument393 pagesB757-200 MPDSebastian Rendon100% (3)
- Wound Care, Dressing and BandagingDocument11 pagesWound Care, Dressing and BandagingJessica Febrina Wuisan100% (1)
- 11 Biology Notes Ch10 Cell Cycle and Cell DevisionDocument7 pages11 Biology Notes Ch10 Cell Cycle and Cell DevisionRohit ThakranNo ratings yet
- TrajentaDocument23 pagesTrajentamonicaolivineNo ratings yet
- Blood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlDocument8 pagesBlood Pressure Management in Patients With Diabetes: Clinical Trial Evidence For BP ControlNovita WulandariNo ratings yet
- II PUC PHYSICS - Previously Appeared Questions and Answers For 2021 Exam by MANJUNATH BDocument52 pagesII PUC PHYSICS - Previously Appeared Questions and Answers For 2021 Exam by MANJUNATH BVishal Ramesh100% (1)
- Integral CalculusDocument48 pagesIntegral CalculusVincent CortezNo ratings yet
- Manual stack emission monitoring standardDocument29 pagesManual stack emission monitoring standardsantisal11No ratings yet
- Give Me Five 6 Pupils BookDocument129 pagesGive Me Five 6 Pupils BookAdrian Gonzalez100% (5)
- Unmet Needs in Diabetes: Present and Future From Clinical PracticeDocument53 pagesUnmet Needs in Diabetes: Present and Future From Clinical PracticescribdNo ratings yet
- Diabetes Update: Facts Show Growing Prevalence and Costs Despite Intensifying TreatmentDocument28 pagesDiabetes Update: Facts Show Growing Prevalence and Costs Despite Intensifying TreatmentPilar Victoria Arrieta VegaNo ratings yet
- Sitagliptin Slide Set Specialist - 1Document31 pagesSitagliptin Slide Set Specialist - 1Fannia Setiani100% (1)
- Facts on Timber Engineering and StructuresDocument73 pagesFacts on Timber Engineering and StructuresNaresworo NugrohoNo ratings yet
- Lipid Management in The Diabetic PatientDocument32 pagesLipid Management in The Diabetic PatientJezza Estévez VarelaNo ratings yet
- PfutznerDocument41 pagesPfutznermina100% (1)
- From Evidence to Clinical Practice in Diabetes ManagementDocument40 pagesFrom Evidence to Clinical Practice in Diabetes ManagementscribdNo ratings yet
- Glucose Control in Diabetes: Focus On SulfhonylureaDocument93 pagesGlucose Control in Diabetes: Focus On SulfhonylureascribdNo ratings yet
- Insulin Therapy in The Inpatient and Outpatient SettingDocument83 pagesInsulin Therapy in The Inpatient and Outpatient SettingFriedman Diabetes Institute100% (1)
- AtorvastatinDocument27 pagesAtorvastatinBolgam PradeepNo ratings yet
- Building A Diabetes Alliance: The Role of Provider EducationDocument32 pagesBuilding A Diabetes Alliance: The Role of Provider EducationMark ReinhardtNo ratings yet
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNo ratings yet
- 15 Advance TrialDocument35 pages15 Advance TrialShaheen UsmaniNo ratings yet
- Wos Care LipidDocument55 pagesWos Care LipidJuliana FeronNo ratings yet
- Estatinas Riesgo y BeneficioDocument4 pagesEstatinas Riesgo y BeneficioHamandita MoraNo ratings yet
- Insulin in DMDocument46 pagesInsulin in DMask1400No ratings yet
- Heart Diseases: An Overview On Clinical Trials: Dr. Khaled Dhifullah Al-Harby Consultant Family PhysicianDocument68 pagesHeart Diseases: An Overview On Clinical Trials: Dr. Khaled Dhifullah Al-Harby Consultant Family PhysicianalghaidanyNo ratings yet
- UkpdsDocument100 pagesUkpdsBeny Rilianto0% (1)
- Selecting Successful Lipid-Lowering Treatments: James M. Mckenney, PharmdDocument31 pagesSelecting Successful Lipid-Lowering Treatments: James M. Mckenney, Pharmdja30jd15ve15an22No ratings yet
- Acp Sglt2 Slidecast 220Document169 pagesAcp Sglt2 Slidecast 220charanmann9165No ratings yet
- 27 FullDocument6 pages27 FullKrishna R KhanalNo ratings yet
- UKPDS 39 compares atenolol and captoprilDocument8 pagesUKPDS 39 compares atenolol and captoprilLaila MayangsariNo ratings yet
- 1.slide Igp Expo Dr. Aulia EditDocument34 pages1.slide Igp Expo Dr. Aulia EditNita Juliana AnggrainiNo ratings yet
- Manajemen Hipertensi Pada Penyakit JantungDocument57 pagesManajemen Hipertensi Pada Penyakit JantungAnonymous nhaFUpOLNo ratings yet
- Cardio Metabolic Risk in DiabetesDocument29 pagesCardio Metabolic Risk in DiabetesoctoindradjajaNo ratings yet
- Secondary Prevention Slide Set: AHA Stroke Guideline 2006Document42 pagesSecondary Prevention Slide Set: AHA Stroke Guideline 2006NEuRoLoGisT CoFFeeCuP100% (1)
- Basal Vs. Pre-Mix Insulin: A ComparisonDocument61 pagesBasal Vs. Pre-Mix Insulin: A Comparisonrajkumar_lalwaniNo ratings yet
- Intensive BloodDocument2 pagesIntensive BloodHyderNo ratings yet
- UKPDSDocument39 pagesUKPDSIsaac TellezNo ratings yet
- TEACHING OF DIABETES MELLITUSDocument4 pagesTEACHING OF DIABETES MELLITUSpearl_nursingNo ratings yet
- Present Therapies of Type 2 Diabetes Mellitus: ACP Annual Session MTP 057&058 San Francisco, CA April 15-16, 2005Document127 pagesPresent Therapies of Type 2 Diabetes Mellitus: ACP Annual Session MTP 057&058 San Francisco, CA April 15-16, 2005Noorhayati Bt Osman NoorhayatiNo ratings yet
- Weight Loss Drug Cutting Risk of Heart AttackDocument12 pagesWeight Loss Drug Cutting Risk of Heart AttackWKYC.comNo ratings yet
- Objective:: BackgroundDocument23 pagesObjective:: BackgroundJanine DimaangayNo ratings yet
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionFrom EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionNo ratings yet
- Semaglutide and Cardiovascular Outcomes in Obesity Without DiabetesDocument12 pagesSemaglutide and Cardiovascular Outcomes in Obesity Without Diabetesmengyanli.528No ratings yet
- Intensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialDocument4 pagesIntensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialSheebaNo ratings yet
- Pharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyDocument37 pagesPharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyKevin JiaNo ratings yet
- Management of Diabetes Mellitus in Patients With Chronic Kidney DiseaseDocument9 pagesManagement of Diabetes Mellitus in Patients With Chronic Kidney DiseasezakyNo ratings yet
- Busting The Myth of Saturated Fat in Heart Disease British Medical Journal 2013Document2 pagesBusting The Myth of Saturated Fat in Heart Disease British Medical Journal 2013jackjensen2852No ratings yet
- Statin Evolution Evidence, Efficacy and ExperienceDocument59 pagesStatin Evolution Evidence, Efficacy and ExperienceSheikh Sharfuddin RajeevNo ratings yet
- Preventing Cardiovascular Disease in Patients With.2 PDFDocument3 pagesPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010No ratings yet
- 2016 Article 69Document10 pages2016 Article 69Rhowy Al-mu'izzahNo ratings yet
- Kelompok 7 - Obat Yang Mempengaruhi Metabolisme LipidDocument5 pagesKelompok 7 - Obat Yang Mempengaruhi Metabolisme LipidNurika ListyanNo ratings yet
- Diamicron MRDocument50 pagesDiamicron MROmar Kamel Rayyan33% (3)
- MRC/BHF Heart Protection Study of Cholesterol Lowering With Simvastatin in 20 536 High-Risk Individuals: A Randomised Placebocontrolled TrialDocument16 pagesMRC/BHF Heart Protection Study of Cholesterol Lowering With Simvastatin in 20 536 High-Risk Individuals: A Randomised Placebocontrolled Trialblopper123No ratings yet
- 10 12 16 Journal Club ExampleDocument52 pages10 12 16 Journal Club ExampleSandra BaiNo ratings yet
- EBP Article 5Document7 pagesEBP Article 5awuahbohNo ratings yet
- 6 Studii StatineDocument37 pages6 Studii Statinejust4uhopeNo ratings yet
- Management of Hyperglycemia and Diabetes in The HospitalDocument46 pagesManagement of Hyperglycemia and Diabetes in The HospitalvinoadhiyogaNo ratings yet
- JNC 8: What changes may be in store for hypertension guidelinesDocument47 pagesJNC 8: What changes may be in store for hypertension guidelinesDavid Chandra EriksonNo ratings yet
- Effects of Medical Therapies On Retinopathy Progression in Type 2 DiabetesDocument12 pagesEffects of Medical Therapies On Retinopathy Progression in Type 2 DiabetesLutfi MalefoNo ratings yet
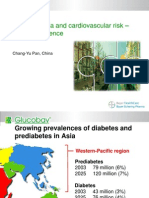
- Asia - Pan - Dysglycaemia and Cardiovascular Risk Û Asian ExperienceDocument18 pagesAsia - Pan - Dysglycaemia and Cardiovascular Risk Û Asian ExperienceputrakartonoNo ratings yet
- Correlates of Acute Insulin Resistance in The Early Phase of Non-Diabetic ST-elevation Myocardial InfarctionDocument9 pagesCorrelates of Acute Insulin Resistance in The Early Phase of Non-Diabetic ST-elevation Myocardial InfarctionmeliabudiNo ratings yet
- Dia Care-2005-Sever-1151-7Document7 pagesDia Care-2005-Sever-1151-7Barbara Sakura RiawanNo ratings yet
- Diabetes and Cardiovascular DiseaseDocument119 pagesDiabetes and Cardiovascular DiseaseAlina PopaNo ratings yet
- Meeting the American Diabetes Association Standards of Care: An Algorithmic Approach to Clinical Care of the Diabetes PatientFrom EverandMeeting the American Diabetes Association Standards of Care: An Algorithmic Approach to Clinical Care of the Diabetes PatientNo ratings yet
- Wiring Harness Installation Instructions: For InstallersDocument12 pagesWiring Harness Installation Instructions: For Installersnirut_niceguyNo ratings yet
- Zaldivar Et Al. 2017 (Dopamine Is Signaled by Mid-Frequency Oscillations and Boosts Output Layers Visual Information in Visual Cortex)Document30 pagesZaldivar Et Al. 2017 (Dopamine Is Signaled by Mid-Frequency Oscillations and Boosts Output Layers Visual Information in Visual Cortex)FRANCISCO ELI LEZAMA GUTIERREZNo ratings yet
- Phylum Chordata TransesDocument2 pagesPhylum Chordata TransesMaribel Ramos InterinoNo ratings yet
- Persian Polymath Physician Al-Rāzī's Life and WorksDocument10 pagesPersian Polymath Physician Al-Rāzī's Life and WorksAnonymous 29PN6AZTNo ratings yet
- Berry phase in the simple harmonic oscillatorDocument14 pagesBerry phase in the simple harmonic oscillatora2618765No ratings yet
- Form Vs Content in P.K. Dick's The Father ThingDocument4 pagesForm Vs Content in P.K. Dick's The Father ThingFrank BertrandNo ratings yet
- Circulation 2006 Boyle 339 52 PDFDocument21 pagesCirculation 2006 Boyle 339 52 PDFSherlocknovNo ratings yet
- Off Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Document2 pagesOff Road and Military Vehicles Off Road Vehicles Agrale Marruaam200 1Victor SilvaNo ratings yet
- VTBS 20-3DDocument1 pageVTBS 20-3Dwong keen faivNo ratings yet
- Syngo MR E11 OncoDocument64 pagesSyngo MR E11 OncoLuís GuerraNo ratings yet
- Assessing A Peripheral PulseDocument5 pagesAssessing A Peripheral Pulsecrrfrnc0% (1)
- TN 015 Overrides 15Document8 pagesTN 015 Overrides 15Luis SantosNo ratings yet
- 12.3 Operation Qualification Protocol For Laminar Air Flow UnitDocument4 pages12.3 Operation Qualification Protocol For Laminar Air Flow UnituzairNo ratings yet
- D.K.Pandey: Lecture 1: Growth and Decay of Current in RL CircuitDocument5 pagesD.K.Pandey: Lecture 1: Growth and Decay of Current in RL CircuitBBA UniversityNo ratings yet
- PHYS205 Matlab Lab TasksDocument4 pagesPHYS205 Matlab Lab TasksjacobNo ratings yet
- Parts of the Globe: Prime Meridian, Equator and Climate ZonesDocument18 pagesParts of the Globe: Prime Meridian, Equator and Climate Zonesmelgazar tanjayNo ratings yet
- Taylor Ebooks 4 Web 0218Document360 pagesTaylor Ebooks 4 Web 0218aquahellNo ratings yet
- Sunningdale School Notes Summer 2022Document12 pagesSunningdale School Notes Summer 2022sunningdaleschoolNo ratings yet
- Chapter11 Part1 PDFDocument40 pagesChapter11 Part1 PDFvampanezezNo ratings yet