
Dave Dysrhythmias
Dave Dysrhythmias
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Charles Kane Dothraki - Writing Task-1Document2 pagesCharles Kane Dothraki - Writing Task-1jykaganda-2772100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
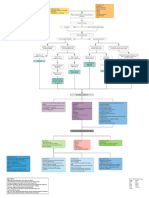
- Myocardial Infarction With CABG Concept MapDocument1 pageMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- Chapter 31 - Assessment and Management of Patients With Vascular DisordersDocument7 pagesChapter 31 - Assessment and Management of Patients With Vascular DisordersMichael Boado100% (1)
- Wound Management: Using Levine's Conservation Model To Guide PracticeDocument6 pagesWound Management: Using Levine's Conservation Model To Guide PracticeGedeAriyanaKusumaNo ratings yet
- Test Bank For Interpreting Ecgs A Practical Approach 3rd Edition Bruce ShadeDocument11 pagesTest Bank For Interpreting Ecgs A Practical Approach 3rd Edition Bruce ShadeLisaTurnerMDkfym100% (30)
- Transient Ischemic AttackDocument23 pagesTransient Ischemic AttackAnonymous 9xHTwHYNo ratings yet
- Association Rule Mining To Detect Factors Which Contribute To Heart Disease in Males and Females 2013Document8 pagesAssociation Rule Mining To Detect Factors Which Contribute To Heart Disease in Males and Females 2013Great Ideas in 5 Minutes افكارعظيمة في 5 دقائقNo ratings yet
- Anatomic Exposures For Vascular Surgery 2013 PDFDocument604 pagesAnatomic Exposures For Vascular Surgery 2013 PDFLiz Eth Chavez100% (4)
- Terapi CompressionDocument10 pagesTerapi CompressionErlinda KarimNo ratings yet
- Peripartum Cardiomyopathy ReviewDocument14 pagesPeripartum Cardiomyopathy ReviewWalter Saavedra Yarleque100% (1)
- Coronary Heart DiseaseDocument8 pagesCoronary Heart Diseasepaul vinothNo ratings yet
- Coronary Artery Diseases - Ilham PDocument43 pagesCoronary Artery Diseases - Ilham PKeputrian FKUPNo ratings yet
- ECG Interpretation BookDocument57 pagesECG Interpretation BookLouis Plan100% (2)
- Kapur 2015Document4 pagesKapur 2015SuhartiniNo ratings yet
- Renovascular Hypertension (RVH) SeminarDocument58 pagesRenovascular Hypertension (RVH) SeminarfaizalmasoodiNo ratings yet
- Quick Reference Guide IAB Insertion CS300 Operation ENDocument36 pagesQuick Reference Guide IAB Insertion CS300 Operation ENCatherine MorrisNo ratings yet
- Dizziness and Loss of Consciousness: Cardiovascular CausesDocument4 pagesDizziness and Loss of Consciousness: Cardiovascular CausesMohammedNo ratings yet
- 2020 - Cardiovascular Effects of Sodium-Glucose Cotransporter-2 Inhibitors in Adults With Type 2 DiabetesDocument7 pages2020 - Cardiovascular Effects of Sodium-Glucose Cotransporter-2 Inhibitors in Adults With Type 2 DiabetesWENDY JOHANA HENRIQUEZ SEGURA ESTUDIANTE ACTIVONo ratings yet
- NCP (Coronary Artery Disease) - PacateDocument7 pagesNCP (Coronary Artery Disease) - PacateKristile Ann PacateNo ratings yet
- Nursing Seminar 1 SAS Session 21Document9 pagesNursing Seminar 1 SAS Session 21ZiaNo ratings yet
- Scientech 2357: Scope of LearningDocument1 pageScientech 2357: Scope of LearningSudip KunduNo ratings yet
- Symptoms of CvsDocument25 pagesSymptoms of CvsstudymedicNo ratings yet
- 2021 ESC Prevencija KV BolestiDocument72 pages2021 ESC Prevencija KV BolestiМилан ЛабудовићNo ratings yet
- Sample Report Alpha DogDocument130 pagesSample Report Alpha DogUsman DastgirNo ratings yet
- Contents of Blood: Unit 1.2: Fluids!Document4 pagesContents of Blood: Unit 1.2: Fluids!Elise NovaNo ratings yet
- Vspo 1 100Document83 pagesVspo 1 100calchasNo ratings yet
- Chapter-5 - Unit-1 - Pharmacognosy: LaxativesDocument9 pagesChapter-5 - Unit-1 - Pharmacognosy: LaxativesAaQib Ali RaZaNo ratings yet
- "Myocardial Infarction": Case StudyDocument36 pages"Myocardial Infarction": Case StudyJosh100% (1)
- NEUROANATOMY Lecture # 07 (BLOOD SUPPLY OF CNS)Document26 pagesNEUROANATOMY Lecture # 07 (BLOOD SUPPLY OF CNS)MISS. COMNo ratings yet
- Case Study On Ob Ward PreeclampsiaDocument12 pagesCase Study On Ob Ward PreeclampsiaNimrod83% (6)




































































You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Charles Kane Dothraki - Writing Task-1Document2 pagesCharles Kane Dothraki - Writing Task-1jykaganda-2772100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Myocardial Infarction With CABG Concept MapDocument1 pageMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- Chapter 31 - Assessment and Management of Patients With Vascular DisordersDocument7 pagesChapter 31 - Assessment and Management of Patients With Vascular DisordersMichael Boado100% (1)
- Wound Management: Using Levine's Conservation Model To Guide PracticeDocument6 pagesWound Management: Using Levine's Conservation Model To Guide PracticeGedeAriyanaKusumaNo ratings yet
- Test Bank For Interpreting Ecgs A Practical Approach 3rd Edition Bruce ShadeDocument11 pagesTest Bank For Interpreting Ecgs A Practical Approach 3rd Edition Bruce ShadeLisaTurnerMDkfym100% (30)
- Transient Ischemic AttackDocument23 pagesTransient Ischemic AttackAnonymous 9xHTwHYNo ratings yet
- Association Rule Mining To Detect Factors Which Contribute To Heart Disease in Males and Females 2013Document8 pagesAssociation Rule Mining To Detect Factors Which Contribute To Heart Disease in Males and Females 2013Great Ideas in 5 Minutes افكارعظيمة في 5 دقائقNo ratings yet
- Anatomic Exposures For Vascular Surgery 2013 PDFDocument604 pagesAnatomic Exposures For Vascular Surgery 2013 PDFLiz Eth Chavez100% (4)
- Terapi CompressionDocument10 pagesTerapi CompressionErlinda KarimNo ratings yet
- Peripartum Cardiomyopathy ReviewDocument14 pagesPeripartum Cardiomyopathy ReviewWalter Saavedra Yarleque100% (1)
- Coronary Heart DiseaseDocument8 pagesCoronary Heart Diseasepaul vinothNo ratings yet
- Coronary Artery Diseases - Ilham PDocument43 pagesCoronary Artery Diseases - Ilham PKeputrian FKUPNo ratings yet
- ECG Interpretation BookDocument57 pagesECG Interpretation BookLouis Plan100% (2)
- Kapur 2015Document4 pagesKapur 2015SuhartiniNo ratings yet
- Renovascular Hypertension (RVH) SeminarDocument58 pagesRenovascular Hypertension (RVH) SeminarfaizalmasoodiNo ratings yet
- Quick Reference Guide IAB Insertion CS300 Operation ENDocument36 pagesQuick Reference Guide IAB Insertion CS300 Operation ENCatherine MorrisNo ratings yet
- Dizziness and Loss of Consciousness: Cardiovascular CausesDocument4 pagesDizziness and Loss of Consciousness: Cardiovascular CausesMohammedNo ratings yet
- 2020 - Cardiovascular Effects of Sodium-Glucose Cotransporter-2 Inhibitors in Adults With Type 2 DiabetesDocument7 pages2020 - Cardiovascular Effects of Sodium-Glucose Cotransporter-2 Inhibitors in Adults With Type 2 DiabetesWENDY JOHANA HENRIQUEZ SEGURA ESTUDIANTE ACTIVONo ratings yet
- NCP (Coronary Artery Disease) - PacateDocument7 pagesNCP (Coronary Artery Disease) - PacateKristile Ann PacateNo ratings yet
- Nursing Seminar 1 SAS Session 21Document9 pagesNursing Seminar 1 SAS Session 21ZiaNo ratings yet
- Scientech 2357: Scope of LearningDocument1 pageScientech 2357: Scope of LearningSudip KunduNo ratings yet
- Symptoms of CvsDocument25 pagesSymptoms of CvsstudymedicNo ratings yet
- 2021 ESC Prevencija KV BolestiDocument72 pages2021 ESC Prevencija KV BolestiМилан ЛабудовићNo ratings yet
- Sample Report Alpha DogDocument130 pagesSample Report Alpha DogUsman DastgirNo ratings yet
- Contents of Blood: Unit 1.2: Fluids!Document4 pagesContents of Blood: Unit 1.2: Fluids!Elise NovaNo ratings yet
- Vspo 1 100Document83 pagesVspo 1 100calchasNo ratings yet
- Chapter-5 - Unit-1 - Pharmacognosy: LaxativesDocument9 pagesChapter-5 - Unit-1 - Pharmacognosy: LaxativesAaQib Ali RaZaNo ratings yet
- "Myocardial Infarction": Case StudyDocument36 pages"Myocardial Infarction": Case StudyJosh100% (1)
- NEUROANATOMY Lecture # 07 (BLOOD SUPPLY OF CNS)Document26 pagesNEUROANATOMY Lecture # 07 (BLOOD SUPPLY OF CNS)MISS. COMNo ratings yet
- Case Study On Ob Ward PreeclampsiaDocument12 pagesCase Study On Ob Ward PreeclampsiaNimrod83% (6)