You might also like
- Hip Flexors - The Iliopsoas - Tightness or WeaknessDocument4 pagesHip Flexors - The Iliopsoas - Tightness or Weaknessatpicker100% (1)
- Sacroiliac Joint Dysfunction and Piriformis Syndrome PDFDocument37 pagesSacroiliac Joint Dysfunction and Piriformis Syndrome PDFDevi SiswaniNo ratings yet
- Canine Parvovirus Fact Sheet 2018-07-0Document5 pagesCanine Parvovirus Fact Sheet 2018-07-0WDIV/ClickOnDetroitNo ratings yet
- Trunk Stabilization ProgramDocument20 pagesTrunk Stabilization ProgramLate ArtistNo ratings yet
- Lecture 1: Lumbar: Indirect ObjectivesDocument11 pagesLecture 1: Lumbar: Indirect ObjectiveseugeniaNo ratings yet
- Lower Crossed SyndromeDocument11 pagesLower Crossed SyndromeJúnior Alvacir Camargo50% (2)
- I. Etiology Primary Adhesive Capsulitis Secondary Adhesive CapsulitisDocument8 pagesI. Etiology Primary Adhesive Capsulitis Secondary Adhesive CapsulitisVanessa Yvonne Gurtiza100% (1)
- Run With No Pain: A Step-by-Step Exercise Solution for Eliminating Low Back Pain in AthletesFrom EverandRun With No Pain: A Step-by-Step Exercise Solution for Eliminating Low Back Pain in AthletesNo ratings yet
- Low Back PainDocument100 pagesLow Back Painchandrusai100% (1)
- Approach To A Patient With Low Back Ache: DR - Ankur BatraDocument104 pagesApproach To A Patient With Low Back Ache: DR - Ankur BatraAnkur Batra100% (1)
- Approach To Lower Back Pain and RadiculopathyDocument54 pagesApproach To Lower Back Pain and Radiculopathyapi-635609849No ratings yet
- Spondylolysis SpondylolisthesisDocument89 pagesSpondylolysis SpondylolisthesisAh ZhangNo ratings yet
- Micronutrients in Neurology and DiseaseDocument16 pagesMicronutrients in Neurology and DiseaseSrinivas PingaliNo ratings yet
- Lower Crossed SyndromeDocument8 pagesLower Crossed SyndromeThaseen75% (4)
- LBP in Pregnancy: OMT For The MDDocument23 pagesLBP in Pregnancy: OMT For The MDOkimi Suyi JuliusNo ratings yet
- Rotator Cuff TendinitisDocument23 pagesRotator Cuff TendinitisVrushali NikamNo ratings yet
- Shoulder Impinge MentDocument26 pagesShoulder Impinge MentkotraeNo ratings yet
- 14 Day Activity Challenge PDFDocument4 pages14 Day Activity Challenge PDFNaila AfzalNo ratings yet
- Ankylosing SpondylitisDocument31 pagesAnkylosing SpondylitisArathy100% (1)
- 9 Hip & Lumber DDDocument29 pages9 Hip & Lumber DDHeba Abo bakrNo ratings yet
- LOW Back Pain: Pamela Rockwell, DODocument57 pagesLOW Back Pain: Pamela Rockwell, DODania ZaidNo ratings yet
- Geriatric PsychiatryDocument27 pagesGeriatric PsychiatryJosephine IrenaNo ratings yet
- Cure Your Back Pain - The Complete Guide to Getting Rid Of Your Back PainFrom EverandCure Your Back Pain - The Complete Guide to Getting Rid Of Your Back PainNo ratings yet
- 3 Letter Guess The Word PDFDocument59 pages3 Letter Guess The Word PDFNaila AfzalNo ratings yet
- Ethical, Legal, Psychosocial Issues in GeneticDocument68 pagesEthical, Legal, Psychosocial Issues in GeneticShalini ChanduNo ratings yet
- TendinitisDocument7 pagesTendinitisIceLeg SamUelNo ratings yet
- Lumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuDocument38 pagesLumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuKapil LakhwaraNo ratings yet
- Pediatric AssessmentDocument9 pagesPediatric AssessmentBea SamonteNo ratings yet
- Ischemic Stroke Case StudyDocument33 pagesIschemic Stroke Case StudyYanne Barrido89% (19)
- Lumbar Disc HerniationDocument8 pagesLumbar Disc Herniationandra_scooterNo ratings yet
- b53 Swasa Kosa Mudra 07Document3 pagesb53 Swasa Kosa Mudra 07shadowfalcon03No ratings yet
- PathoConceptMap AIDSDocument3 pagesPathoConceptMap AIDSKristen Babauta50% (2)
- Small For Gestational AgeDocument14 pagesSmall For Gestational AgeMaria Delia Salvado100% (2)
- Ortho DR - RehabDocument44 pagesOrtho DR - RehabMohammed Saad NabhanNo ratings yet
- ICD-9-CM Code: 724.3 ICF CodesDocument8 pagesICD-9-CM Code: 724.3 ICF CodesGeorgiana MilcoveanuNo ratings yet
- Lec7 Assessment of SpineDocument35 pagesLec7 Assessment of Spinesana mumtazNo ratings yet
- Lumbo-Pelvic Stability and Back Pain: What's The Link?Document8 pagesLumbo-Pelvic Stability and Back Pain: What's The Link?atul-heroNo ratings yet
- Case ReportDocument14 pagesCase Reportapi-678217089No ratings yet
- ScoliosesDocument10 pagesScolioseschandiwalaNo ratings yet
- Exercise 1Document4 pagesExercise 1api-479716004No ratings yet
- Lower Crossed SyndromeDocument5 pagesLower Crossed SyndromeD. HrmsNo ratings yet
- Physical Therapy in Lumbar SpineDocument12 pagesPhysical Therapy in Lumbar SpineMarcos Perez AlbertNo ratings yet
- Major ProjectDocument10 pagesMajor Projectbharath rajNo ratings yet
- Exercise 1Document6 pagesExercise 1api-455408952No ratings yet
- Week 4 ExerciseDocument5 pagesWeek 4 Exerciseapi-467743065No ratings yet
- Assessmentofshoulder 180107041721Document36 pagesAssessmentofshoulder 180107041721Chandra PrabhaNo ratings yet
- Supervised Clinical Practice-III: AssignmentDocument12 pagesSupervised Clinical Practice-III: Assignmentzainab siddiqueNo ratings yet
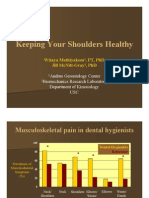
- Keeping Your Shoulders HealthyDocument38 pagesKeeping Your Shoulders Healthyxyz84No ratings yet
- Ankylosing SpondylytisDocument6 pagesAnkylosing SpondylytisMurad KurdiNo ratings yet
- In Service PresentationDocument15 pagesIn Service Presentationapi-661490009No ratings yet
- Refrat Remato LBPDocument33 pagesRefrat Remato LBPwulanNo ratings yet
- Spine Stabilization PowerpointDocument87 pagesSpine Stabilization PowerpointALLAN COSTA MONTEIRONo ratings yet
- WK 6 Study QsDocument7 pagesWK 6 Study Qsapi-479720222No ratings yet
- Lower Back Pain 2Document39 pagesLower Back Pain 2joe BouGhazaliNo ratings yet
- Brunnstorm ApproachDocument70 pagesBrunnstorm Approachkomal khannaNo ratings yet
- Inflammatory Disorders E.G. (Ankylosing Spondylitis) Spondylolisthesis Radiculopathies ArthrosesDocument5 pagesInflammatory Disorders E.G. (Ankylosing Spondylitis) Spondylolisthesis Radiculopathies Arthrosesapi-477982644No ratings yet
- Abnormal Changes in GaitDocument6 pagesAbnormal Changes in GaitVilakshan RaajNo ratings yet
- Tutorial Low Back Pain: Rahma Herviastuti 12/329221/KU/14991 Pembimbing: Dr. Wahyu Wihartono, SP.S, M.KesDocument40 pagesTutorial Low Back Pain: Rahma Herviastuti 12/329221/KU/14991 Pembimbing: Dr. Wahyu Wihartono, SP.S, M.KesRahma HerviastutiNo ratings yet
- Exercitii ReabilitareDocument5 pagesExercitii ReabilitareGabriela Istrati-StanciugelNo ratings yet
- DC 66 Local StabilizersDocument4 pagesDC 66 Local StabilizersErik BeijerNo ratings yet
- William 2Document15 pagesWilliam 2Jenny VibsNo ratings yet
- Patellofemoral/Chondromalacia Protocol: Anatomy and BiomechanicsDocument8 pagesPatellofemoral/Chondromalacia Protocol: Anatomy and BiomechanicsGirijashankar KhuntiaNo ratings yet
- Patellofemoral/Chondromalacia Protocol: Anatomy and BiomechanicsDocument8 pagesPatellofemoral/Chondromalacia Protocol: Anatomy and BiomechanicsRia PuputNo ratings yet
- 10, Pain Management of Spinalcord Injury-1Document23 pages10, Pain Management of Spinalcord Injury-1Zeeshan AhmadNo ratings yet
- Week 6Document8 pagesWeek 6api-479499469No ratings yet
- Path Gait 1 OrthoDocument8 pagesPath Gait 1 OrthoMauricio AlexisNo ratings yet
- All ThesisDocument113 pagesAll ThesisImraan KhanNo ratings yet
- Herniated Nucleus PulposusDocument29 pagesHerniated Nucleus PulposusRussel JanoloNo ratings yet
- WikipediaDocument1 pageWikipediaMizsh AguilanNo ratings yet
- Holistic Home Remedies for Acute Low Back Pain: Incorporating Stretching and the McKenzie MethodFrom EverandHolistic Home Remedies for Acute Low Back Pain: Incorporating Stretching and the McKenzie MethodNo ratings yet
- Science Lecture 2Document25 pagesScience Lecture 2Naila AfzalNo ratings yet
- 1st KalmaDocument6 pages1st KalmaNaila AfzalNo ratings yet
- The Sabbath BreakerDocument25 pagesThe Sabbath BreakerNaila AfzalNo ratings yet
- Clean Eating Diet PlanDocument2 pagesClean Eating Diet PlanNaila AfzalNo ratings yet
- BoliviaDocument4 pagesBoliviaNaila AfzalNo ratings yet
- P2Lkids Tarbiyah Camp: We Do Things Differently Becoz .We Are Different ! MathDocument1 pageP2Lkids Tarbiyah Camp: We Do Things Differently Becoz .We Are Different ! MathNaila AfzalNo ratings yet
- Busyspider C PDFDocument11 pagesBusyspider C PDFNaila AfzalNo ratings yet
- EnglishNursery Aa1e43f3Document11 pagesEnglishNursery Aa1e43f3Naila AfzalNo ratings yet
- 4 6 PDFDocument1 page4 6 PDFNaila AfzalNo ratings yet
- P2Lkids Tarbiyah Camp 2020: Ethics Story: Obey Your ParentsDocument1 pageP2Lkids Tarbiyah Camp 2020: Ethics Story: Obey Your ParentsNaila AfzalNo ratings yet
- P2Lkids Tarbiyah CampDocument1 pageP2Lkids Tarbiyah CampNaila AfzalNo ratings yet
- 4 6 PDFDocument1 page4 6 PDFNaila AfzalNo ratings yet
- P2Lkids Tarbiyah Camp 2020: MyselfDocument1 pageP2Lkids Tarbiyah Camp 2020: MyselfNaila AfzalNo ratings yet
- P2Lkids Tarbiyah Camp 2020: Ethics Story: Obey Your ParentsDocument1 pageP2Lkids Tarbiyah Camp 2020: Ethics Story: Obey Your ParentsNaila AfzalNo ratings yet
- P2Lkids Tarbiyah CampDocument1 pageP2Lkids Tarbiyah CampNaila AfzalNo ratings yet
- P2Lkids Tarbiyah Camp: We Do Things Differently Becoz .We Are Different ! Ethics Video TaskDocument1 pageP2Lkids Tarbiyah Camp: We Do Things Differently Becoz .We Are Different ! Ethics Video TaskNaila AfzalNo ratings yet
- Banana Diet Plan: InstructionsDocument1 pageBanana Diet Plan: InstructionsNaila AfzalNo ratings yet
- Common Complications of Active TuberculosisDocument2 pagesCommon Complications of Active TuberculosisNaila AfzalNo ratings yet
- Daniel Santiago Rincón PinzónDocument2 pagesDaniel Santiago Rincón PinzónYANDRA YINNETH RINCON PINZONNo ratings yet
- Pathology & Clinical Laboratory (M) SDN - BHD: Scan QR For VerificationDocument1 pagePathology & Clinical Laboratory (M) SDN - BHD: Scan QR For VerificationAzhar SabriNo ratings yet
- Risk Factors of Hearing Defects and Their Relationship To The Outcome of Hearing Screening Among NeonatesDocument6 pagesRisk Factors of Hearing Defects and Their Relationship To The Outcome of Hearing Screening Among NeonatesRendra SyaniNo ratings yet
- Department of Education: Science IvDocument2 pagesDepartment of Education: Science IvCristita Macaranas Vigo100% (1)
- Complex Torch Si SarcinaDocument23 pagesComplex Torch Si SarcinamoldoveanuNo ratings yet
- Seattle Angina QuestionnaireDocument6 pagesSeattle Angina QuestionnaireAmelia SianiparNo ratings yet
- Congenital Syphilis Treatment and PreventionDocument1 pageCongenital Syphilis Treatment and PreventionMuhammad Naufal FadhillahNo ratings yet
- Assessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationCrissa AngelNo ratings yet
- BEER CriteriaDocument9 pagesBEER CriteriaKath EstradaNo ratings yet
- Salmonellosis: Odsigue, Clarissa Rama, Alea Albert Rosales, Joy SybilDocument36 pagesSalmonellosis: Odsigue, Clarissa Rama, Alea Albert Rosales, Joy SybilAleya Albert RamaNo ratings yet
- Cytojournal: Time For Evidence-Based CytologyDocument10 pagesCytojournal: Time For Evidence-Based CytologyAtikah RahmadhaniNo ratings yet
- Diagnosis and TreatmentDocument6 pagesDiagnosis and TreatmentVadim BulbakNo ratings yet
- Cushing - AddisonDocument27 pagesCushing - AddisonMelissa-Andreea Ardeleanu Carvajal OsorioNo ratings yet
- 25. London Cancer Guidelines for Administration of Systematic Anti-Cancer Therapy-محولDocument106 pages25. London Cancer Guidelines for Administration of Systematic Anti-Cancer Therapy-محولAnsam MohNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale EvaluationDocument6 pagesAssessment Nursing Diagnosis Background Knowledge Planning Intervention Rationale EvaluationMaye ArugayNo ratings yet
- CPSP Demo Mcqs - 2022Document24 pagesCPSP Demo Mcqs - 2022Farhan AfzalNo ratings yet
- DiclofenacDocument3 pagesDiclofenacapi-37979410% (1)
- Advancesinlocal Anesthesiain Dentistry: Orrett E. Ogle,, Ghazal MahjoubiDocument19 pagesAdvancesinlocal Anesthesiain Dentistry: Orrett E. Ogle,, Ghazal Mahjoubicarlos gilbertoNo ratings yet
- Meatotomy and Wound CareDocument13 pagesMeatotomy and Wound CareAgung IndraNo ratings yet
- Urineanalysis PDFDocument68 pagesUrineanalysis PDFztanga7@yahoo.comNo ratings yet
- VATER VACTERL Association and Caudal Regression WithDocument10 pagesVATER VACTERL Association and Caudal Regression WithTatiana OrdoñezNo ratings yet