You might also like
- All EWM TcodesDocument8 pagesAll EWM TcodesgopalNo ratings yet
- Lgu - ScmarDocument12 pagesLgu - ScmarWinalyn LizardoNo ratings yet
- Safe Closure and Rehabilitation Plan of CDO City - Controlled DumpsiteDocument29 pagesSafe Closure and Rehabilitation Plan of CDO City - Controlled DumpsiteEdson Tandoc III100% (3)
- Safe Closure and Rehabilation of Disposal Facilities1Document27 pagesSafe Closure and Rehabilation of Disposal Facilities1Melvin VillanuevaNo ratings yet
- AIP Blank Form 2020Document1 pageAIP Blank Form 2020Johara Soriano0% (1)
- Eo Municipal Land Use CommitteeDocument2 pagesEo Municipal Land Use CommitteeSi-kuya JibbNo ratings yet
- E WasteDocument25 pagesE Wasteanandpwaindeshkar86% (14)
- DA DRRM Operations Manual Part IDocument107 pagesDA DRRM Operations Manual Part IDA 11 DRRNo ratings yet
- Draft EODocument3 pagesDraft EOKim Claidy Lopez100% (2)
- Updated Ten Year Ecological Solid Waste Management PlanDocument142 pagesUpdated Ten Year Ecological Solid Waste Management PlanTrisha DamianNo ratings yet
- Different Classifications of Disposal FacilitiesDocument25 pagesDifferent Classifications of Disposal FacilitiesJM Flores De SilvaNo ratings yet
- BPLS OrdinanceDocument5 pagesBPLS OrdinanceJin SiclonNo ratings yet
- 2023 SGLG Technical Notes - As of 06 June 2023Document134 pages2023 SGLG Technical Notes - As of 06 June 2023Ann ManaloconNo ratings yet
- Annex B. Form 1d Ldis RapidsDocument11 pagesAnnex B. Form 1d Ldis RapidsFender Boyang100% (1)
- Road Clearing 2.0Document31 pagesRoad Clearing 2.0gulp_burp100% (1)
- Form 2E KUMALARANG (Complete)Document10 pagesForm 2E KUMALARANG (Complete)CA T HeNo ratings yet
- POC Secretariat Report 202Document2 pagesPOC Secretariat Report 202DILG STA MARIA100% (1)
- Individual Performance Commitment and Review (Ipcr) : Reviewed: Date Approved byDocument28 pagesIndividual Performance Commitment and Review (Ipcr) : Reviewed: Date Approved byLorna U. Fernandez-EspinozaNo ratings yet
- Waste Analysis and Characterization Study (Wacs) Plan For The Municipality/City Of, 1. ObjectivesDocument25 pagesWaste Analysis and Characterization Study (Wacs) Plan For The Municipality/City Of, 1. ObjectivesAdrian LequiganNo ratings yet
- Ladpa PolicyDocument32 pagesLadpa PolicyShee RealNo ratings yet
- EO On BPLSDocument2 pagesEO On BPLSVinvin EsoenNo ratings yet
- Work and Financial Plan: Nboo-Dilg LCPC Form 001-DDocument2 pagesWork and Financial Plan: Nboo-Dilg LCPC Form 001-DPhong PhongNo ratings yet
- Child Friendly Katarungang PambarangayDocument25 pagesChild Friendly Katarungang PambarangayJaneth Mejia Bautista AlvarezNo ratings yet
- BAC Reso TWG Mt. OliveDocument3 pagesBAC Reso TWG Mt. OliveDon PerfectoNo ratings yet
- Baranggay Disaster Risk Reduction 2018Document44 pagesBaranggay Disaster Risk Reduction 2018David Mikael Nava TaclinoNo ratings yet
- An Order Creating The Water Quality Monitoring Unit of The Municipality of MalapatanDocument3 pagesAn Order Creating The Water Quality Monitoring Unit of The Municipality of MalapatanJoey Coliao100% (5)
- Gawad KALASAG Seal For LDRRMCO Toolkit Guide MR Mario Peralta JRDocument29 pagesGawad KALASAG Seal For LDRRMCO Toolkit Guide MR Mario Peralta JRJosephine Templa-Jamolod100% (1)
- Lgu SWM Scmar 2017 LatestDocument19 pagesLgu SWM Scmar 2017 LatestSean Allen Pagkalinawan100% (1)
- Municipal Solid Waste Project SKTGDocument3 pagesMunicipal Solid Waste Project SKTGDevanSandrasakerenNo ratings yet
- Checklist For 2019 LTIADocument4 pagesChecklist For 2019 LTIAKarl Alava100% (1)
- Certification of RROWDocument4 pagesCertification of RROWGrace Andayran CaingletNo ratings yet
- KP TrainingsDocument6 pagesKP TrainingsJaneth Mejia Bautista AlvarezNo ratings yet
- IPCR July To December 2022Document7 pagesIPCR July To December 2022Decs Del Carmen100% (1)
- Ra 11396Document9 pagesRa 11396Ivy Galit Dula100% (1)
- WACS Plan Template 2-25-19Document32 pagesWACS Plan Template 2-25-19ralp cuya100% (1)
- DILG MC 2019-143 - Omnibus Guidelines On Peace and Order CouncilsDocument130 pagesDILG MC 2019-143 - Omnibus Guidelines On Peace and Order CouncilsDM Patrimonio100% (1)
- Municipal Anti-Drug Abuse CouncilDocument2 pagesMunicipal Anti-Drug Abuse CouncilDong SantosNo ratings yet
- Intro To Sap Transportation Management PDFDocument11 pagesIntro To Sap Transportation Management PDFChye Kian OngNo ratings yet
- Enhanced CDP Assessment Tool BLGD CAT Form 1 BDocument31 pagesEnhanced CDP Assessment Tool BLGD CAT Form 1 Bmpdo calinog100% (2)
- Akta Kualiti Alam Sekitar (Buangan TerjadualDocument25 pagesAkta Kualiti Alam Sekitar (Buangan Terjadualshafie.buang67% (3)
- Basic Information::: Form 1 - Embv - SWM - MRFDocument3 pagesBasic Information::: Form 1 - Embv - SWM - MRFDominic CareoNo ratings yet
- MRF Moa SigningDocument2 pagesMRF Moa SigningYmer VTNo ratings yet
- Activity Design Mini Dump Truck For Solid WasteDocument2 pagesActivity Design Mini Dump Truck For Solid WasteEnp Titus VelezNo ratings yet
- Activity Design - CDP ELADocument3 pagesActivity Design - CDP ELANurah La100% (2)
- Salient Features: Philippine Climate Change ACT - RA 9729Document29 pagesSalient Features: Philippine Climate Change ACT - RA 9729JO HN Scuba-rNo ratings yet
- 5-10yr SWM Plan TemplateDocument27 pages5-10yr SWM Plan TemplateJenni Beth100% (2)
- Form 1 LGU Profile PDFDocument6 pagesForm 1 LGU Profile PDFArt Henrhey Bulic50% (2)
- Anti Smoking Ordinance Poblacion DosDocument4 pagesAnti Smoking Ordinance Poblacion Dosjacquelyn samson100% (1)
- Activity Design WACSDocument4 pagesActivity Design WACSMarie Alejo100% (1)
- LDRRMP Template Description RemarksDocument3 pagesLDRRMP Template Description RemarksLeslie Estorosos33% (3)
- MENRO Creation - AtimonanDocument4 pagesMENRO Creation - AtimonanJohn Francis Luzano100% (1)
- ESWM ReportDocument9 pagesESWM ReportBadidz Ong SucoNo ratings yet
- Project Proposal ADACDocument3 pagesProject Proposal ADACJuan Paolo S. Brosas100% (1)
- E-Waste ManagementDocument18 pagesE-Waste ManagementAnkur PandeyNo ratings yet
- HLURB Schedule of Fees R-912 S 2013 PDFDocument9 pagesHLURB Schedule of Fees R-912 S 2013 PDFcarlsulawNo ratings yet
- ANNEX B. Form 3b Project BriefDocument13 pagesANNEX B. Form 3b Project BriefCattleya PenalosaNo ratings yet
- Municipal Ordinance No. 017-2014Document4 pagesMunicipal Ordinance No. 017-2014SBGuinobatan100% (2)
- Unified LCPC MC (Template Form)Document13 pagesUnified LCPC MC (Template Form)Ian Jun GestaNo ratings yet
- Realignment To Financial AssistanceDocument2 pagesRealignment To Financial AssistanceBarangay Pulo ValenzuelaNo ratings yet
- DR# 2023 MOA-Gov. Uy (Balay Silangan)Document2 pagesDR# 2023 MOA-Gov. Uy (Balay Silangan)Fatima L. MalaluanNo ratings yet
- BDRRM Plan Template EnglishDocument44 pagesBDRRM Plan Template EnglishRodnie AlburoNo ratings yet
- Contingency Planning Checklist For TyphoonsDocument37 pagesContingency Planning Checklist For TyphoonsJuan Carlos GonzalesNo ratings yet
- ELA Activity DesignDocument4 pagesELA Activity DesignAnonymous gP3TAH7W100% (3)
- SCRP BUCLOC LabaanDocument18 pagesSCRP BUCLOC LabaanEmjhay SwakidaNo ratings yet
- A. General Information: Checklist The Closure and Rehabilitation of Open Dumpsites and Controlled DumpsitesDocument5 pagesA. General Information: Checklist The Closure and Rehabilitation of Open Dumpsites and Controlled DumpsitesDM CamilotNo ratings yet
- A. General Information: Checklist The Closure and Rehabilitation of Open Dumpsites and Controlled DumpsitesDocument9 pagesA. General Information: Checklist The Closure and Rehabilitation of Open Dumpsites and Controlled DumpsitesBanta EdmondNo ratings yet
- Initial Environmental Examination (IEE) Checklist ReportDocument10 pagesInitial Environmental Examination (IEE) Checklist ReportavieNo ratings yet
- Industrial PollutionDocument1 pageIndustrial Pollutioncretu_f_deliaNo ratings yet
- Haze Rational ClozeDocument2 pagesHaze Rational ClozePierro De ChivatozNo ratings yet
- Introduction To BioremediationDocument36 pagesIntroduction To BioremediationA. El MahdiNo ratings yet
- Bhiwadi Polymers 3-06-19Document5 pagesBhiwadi Polymers 3-06-19Kaushal KothariNo ratings yet
- Chapter 1 Introduction To Solid WasteDocument2 pagesChapter 1 Introduction To Solid WasteAmeerRashidNo ratings yet
- Awareness of Environmental Pollution and Pollution Control Techniques Among Adults of Kottayam TownDocument3 pagesAwareness of Environmental Pollution and Pollution Control Techniques Among Adults of Kottayam TownAnjumol ShajuNo ratings yet
- ILTDocument2 pagesILTAlexandraNo ratings yet
- TCVN 6772-2000 Waste Water Quality (English Version)Document2 pagesTCVN 6772-2000 Waste Water Quality (English Version)limchNo ratings yet
- EWasteDocument23 pagesEWastesurajsingh85% (20)
- Brief On Basel ConventionDocument1 pageBrief On Basel ConventionAnton SRI PROBIYANTONONo ratings yet
- Reg No 37 1998 Freight Forwarding and Ship Agency LicenseDocument5 pagesReg No 37 1998 Freight Forwarding and Ship Agency Licensebini100% (1)
- Waste ManagementDocument11 pagesWaste ManagementLuis AndersonNo ratings yet
- Reg Update Eng 20150305 PDFDocument2 pagesReg Update Eng 20150305 PDFMarcello CoppolaNo ratings yet
- Joint Affidavit of UndertakingDocument2 pagesJoint Affidavit of UndertakingArnold Cavalida BucoyNo ratings yet
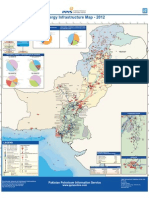
- Energy Map 2012Document1 pageEnergy Map 2012Muhammad Shahid AlamNo ratings yet
- Sig Ferroalloy Fs 052815 PDFDocument3 pagesSig Ferroalloy Fs 052815 PDFeinstein_486No ratings yet
- Chapter 18 Air PollutionDocument47 pagesChapter 18 Air PollutionnavalepeiNo ratings yet
- Inc09 3Document5 pagesInc09 3Hasan Kadir Uçmazoğlu (Student)No ratings yet
- Pirelli Tyres Romania: SlatinaDocument3 pagesPirelli Tyres Romania: SlatinaMihaela VoineaNo ratings yet
- Air Pollution Act 1981Document10 pagesAir Pollution Act 1981RudolfNo ratings yet
- Global Pollution AssignmentDocument5 pagesGlobal Pollution AssignmentAthirah ShafiqueNo ratings yet
- AmkorDocument30 pagesAmkorabcedeNo ratings yet
- Air RegulationsDocument38 pagesAir RegulationsJorn DoeNo ratings yet