You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Internal Medicine Logbook ArabicDocument7 pagesInternal Medicine Logbook ArabicMhmd IrakyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Scoring Rubric For Speaking TestDocument2 pagesScoring Rubric For Speaking Testnur fauziyah89% (18)
- I MCQs Neuro.Document4 pagesI MCQs Neuro.Mhmd Iraky100% (1)
- Orthopaedic Physiotherapy Assessment Chart For Physiotherapists by Dr. Krishna N. SharmaDocument7 pagesOrthopaedic Physiotherapy Assessment Chart For Physiotherapists by Dr. Krishna N. SharmaDr. Krishna N. Sharma86% (58)
- Living From Truth A Manual For Masters of Long Enlightenment IntensivesDocument116 pagesLiving From Truth A Manual For Masters of Long Enlightenment IntensivesZeljko Zex Malinovic100% (1)
- CompreDocument53 pagesCompreGEr JrvillaruEl0% (3)
- Semi Detailed Lesson Plan On Definition and Functions of ManagementDocument4 pagesSemi Detailed Lesson Plan On Definition and Functions of ManagementSydney Lee Macapelit NavaresNo ratings yet
- CV For Project Manager - EngineerDocument4 pagesCV For Project Manager - EngineerShaikh Ibrahim0% (1)
- IER's National Physical Therapy Examination Review & Study Guide2 PDFDocument17 pagesIER's National Physical Therapy Examination Review & Study Guide2 PDFMhmd Iraky0% (1)
- IV. Mcqs NeuroDocument7 pagesIV. Mcqs NeuroMhmd Iraky100% (1)
- III. Mcqs NeuroDocument19 pagesIII. Mcqs NeuroMhmd Iraky100% (2)
- II. MCQs NeuroDocument13 pagesII. MCQs NeuroMhmd Iraky100% (2)
- Balance Assessment and TreatmentDocument55 pagesBalance Assessment and TreatmentMhmd Iraky100% (1)
- ue 1-Broc s Are ʹ an area of the frontal lobe, usually in the left hemisphere, that directs the muscle movements involvedDocument31 pagesue 1-Broc s Are ʹ an area of the frontal lobe, usually in the left hemisphere, that directs the muscle movements involvedMhmd IrakyNo ratings yet
- HVDC Ground ElectrodeDocument13 pagesHVDC Ground ElectrodeHeather CarterNo ratings yet
- Cristalactiv™ Pc105: Ultrafine & Specialty Tio ProductsDocument3 pagesCristalactiv™ Pc105: Ultrafine & Specialty Tio ProductsShweta MahajanNo ratings yet
- 2022 04 01 Vogue SingaporeDocument174 pages2022 04 01 Vogue SingaporeKo KoNo ratings yet
- Prla 2 Set 1 Story - Friends For LifeDocument4 pagesPrla 2 Set 1 Story - Friends For Lifehilmann.ariffinnNo ratings yet
- Notice Machine À CoudreDocument62 pagesNotice Machine À Coudreker lenoNo ratings yet
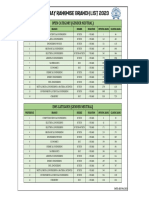
- Iit Bombay Rankwise Branch List 2023Document1 pageIit Bombay Rankwise Branch List 2023Ratan ChoudharyNo ratings yet
- Material Downloaded From - 1 / 6Document6 pagesMaterial Downloaded From - 1 / 6Omprakash ChandrakarNo ratings yet
- Difference Between ISO-IEC 17025 and ISO 10012Document3 pagesDifference Between ISO-IEC 17025 and ISO 10012carlosalejo100% (1)
- The Development of Self-Control of Emotion PDFDocument21 pagesThe Development of Self-Control of Emotion PDFAcelaFloyretteBorregoFabelaNo ratings yet
- MTTM 2nd Year 2019-2 PDFDocument11 pagesMTTM 2nd Year 2019-2 PDFRajnish PathaniaNo ratings yet
- JAVASCRIPT Path FinderDocument98 pagesJAVASCRIPT Path FindernandanNo ratings yet
- (WWW - Asianovel.com) - Liu Yao The Revitalization of Fuyao Sect Vol.1 Chapter 1 - Vol.1 Chapter 8Document77 pages(WWW - Asianovel.com) - Liu Yao The Revitalization of Fuyao Sect Vol.1 Chapter 1 - Vol.1 Chapter 8AnjyNo ratings yet
- Raghunathan 2015Document5 pagesRaghunathan 2015STOCK IKRAM GROUPNo ratings yet
- Emailing Teacher Notes PDFDocument2 pagesEmailing Teacher Notes PDFSylwia WęglewskaNo ratings yet
- Cloud Native Applications in A Telco WorldDocument22 pagesCloud Native Applications in A Telco WorldmarimcuriNo ratings yet
- LP Expert Detective Class 6Document5 pagesLP Expert Detective Class 6Abhishek SumanNo ratings yet
- A Study On Financial Performance Analysis With Reference To TNSC Bank Chennai Ijariie10138Document7 pagesA Study On Financial Performance Analysis With Reference To TNSC Bank Chennai Ijariie10138Jeevitha MuruganNo ratings yet
- Horizon Cardigan UsDocument13 pagesHorizon Cardigan UskerryrobsonstevensonNo ratings yet
- Multiple Integrals: Example 3 SolutionDocument15 pagesMultiple Integrals: Example 3 SolutionshivanshNo ratings yet
- Karishma Project Front PageDocument5 pagesKarishma Project Front PageRohan GargNo ratings yet
- CHEM 1412. Chapter 16. Acids and Bases - Homework - SDocument13 pagesCHEM 1412. Chapter 16. Acids and Bases - Homework - STrisha Anne SyNo ratings yet
- CRSBS BrochureDocument2 pagesCRSBS BrochureKarthik PalaniswamyNo ratings yet
- Compiler LabDocument63 pagesCompiler LabAbhishek YadavNo ratings yet
- Stress-Strain Model of Ultrahigh Performance Concrete Confined by Fiber-Reinforced Polymers, 2013 (Pedram Zohrevand)Document8 pagesStress-Strain Model of Ultrahigh Performance Concrete Confined by Fiber-Reinforced Polymers, 2013 (Pedram Zohrevand)Phan Đào Hoàng HiệpNo ratings yet
- IoT Based Low-Cost Gas Leakage 2020Document6 pagesIoT Based Low-Cost Gas Leakage 2020Sanjevi PNo ratings yet