You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Uc Piqs FinalDocument4 pagesUc Piqs Finalapi-379427121No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
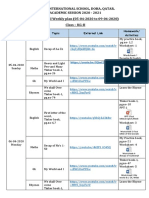
- Loyola International School, Doha, Qatar. Academic Session 2020 - 2021 Home-School Weekly Plan (05-04-2020 To 09-04-2020) Class - KG-IIDocument3 pagesLoyola International School, Doha, Qatar. Academic Session 2020 - 2021 Home-School Weekly Plan (05-04-2020 To 09-04-2020) Class - KG-IIAvik KunduNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Music6 - Q2 - Mod1 - C, G, F MajorDocument40 pagesMusic6 - Q2 - Mod1 - C, G, F MajorJohn Lorenz G. FaltiqueraNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Educating Individuals With Diverse Learning Need1Document8 pagesEducating Individuals With Diverse Learning Need1George OpokuNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Detailed Lesson PlanDocument8 pagesDetailed Lesson PlanSvg Frendz75% (4)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- IBT Practice Test Grade 5 Maths PDFDocument7 pagesIBT Practice Test Grade 5 Maths PDFmamta80% (5)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Cambridge Primary Maths Curriculum OutlineDocument2 pagesCambridge Primary Maths Curriculum OutlineMike Serge Razafi0% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- CSS Monitoring Tool DRRMS Edited 18 Jan 2017 1Document6 pagesCSS Monitoring Tool DRRMS Edited 18 Jan 2017 1Jesse AbabonNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Art TherapyDocument77 pagesArt TherapyMaria Tudosa100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- List of Schools For Special Children in PakistanDocument14 pagesList of Schools For Special Children in Pakistanabedinz100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 8th International Conference On Learning, Education and Pedagogy (LEAP)Document20 pages8th International Conference On Learning, Education and Pedagogy (LEAP)Global Research and Development ServicesNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Supervision in NursingDocument24 pagesSupervision in NursingMakanjuola Osuolale John100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Experts, Semantic and Epistemic: S G Northwestern UniversityDocument18 pagesExperts, Semantic and Epistemic: S G Northwestern UniversityBrian BarreraNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- RPL Mech Eng Proc 05Document20 pagesRPL Mech Eng Proc 05Federico MachedaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- CPHRM Healthcare BrouchureDocument10 pagesCPHRM Healthcare BrouchureHanan AhmedNo ratings yet
- MYP1 Unit-DRAMADocument4 pagesMYP1 Unit-DRAMAMohammad Idreesi100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Agriculture and Fishery ArtsDocument44 pagesAgriculture and Fishery ArtsJohn Ray EnajeNo ratings yet
- Esl Lesson PlanningDocument5 pagesEsl Lesson PlanningAlireza MollaiNo ratings yet
- The Process Audit - Harvard Business ReviewDocument5 pagesThe Process Audit - Harvard Business ReviewAntonio De La Vega OrtegaNo ratings yet
- RUTAGDocument3 pagesRUTAGRidwan AhmedNo ratings yet
- S4 Mitotic Cell Division Lesson Plan PDFDocument4 pagesS4 Mitotic Cell Division Lesson Plan PDFShiella Mae Baltazar BulauitanNo ratings yet
- 11 2f9 6th Grade PLC Agenda and MinutesDocument2 pages11 2f9 6th Grade PLC Agenda and Minutesapi-365464044No ratings yet
- TASK 4 - ELP Assignment (Nur Izatul Atikah)Document7 pagesTASK 4 - ELP Assignment (Nur Izatul Atikah)BNK2062021 Muhammad Zahir Bin Mohd FadleNo ratings yet
- Kester Curriculum VitaeDocument22 pagesKester Curriculum VitaeJohn cenaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Salmonella Reflection PDFDocument2 pagesSalmonella Reflection PDFcNo ratings yet
- CHED E-Forms A B-C Institutional, Programs, Enrollment and Graduates For Private HEIs - AY0910Document7 pagesCHED E-Forms A B-C Institutional, Programs, Enrollment and Graduates For Private HEIs - AY0910ramilsanchez@yahoo.com100% (2)
- Application Form SaumuDocument4 pagesApplication Form SaumuSaumu AbdiNo ratings yet
- Claims of Fact, Policy and ValueDocument7 pagesClaims of Fact, Policy and ValueGreggy LatrasNo ratings yet
- Tutorial Letter FMM3701-2022-S2Document11 pagesTutorial Letter FMM3701-2022-S2leleNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)