You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Ed Coan - Core Manual For Strength Training (Version 2.0)Document40 pagesEd Coan - Core Manual For Strength Training (Version 2.0)blackhawk896% (28)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Goniometry LandmarksDocument2 pagesGoniometry LandmarksBob Grobmyer100% (4)
- Coco Fitness Glute GuideDocument15 pagesCoco Fitness Glute GuideDenise Lomax100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Podiatry Institute ManualDocument301 pagesPodiatry Institute ManualTyler Lawrence Coye100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- An Illustrated Tutorial of Musculoskeletal Sonography Part 1, Introduction - and - General - PrinciplesDocument9 pagesAn Illustrated Tutorial of Musculoskeletal Sonography Part 1, Introduction - and - General - PrinciplesNovitaNo ratings yet
- BCTGuidesFinal Transfusion Perioperatoria PDFDocument11 pagesBCTGuidesFinal Transfusion Perioperatoria PDFMisael Cristián Bustos SáezNo ratings yet
- CDC 5435DS1 PDFDocument211 pagesCDC 5435DS1 PDFbodeadumitru9261No ratings yet
- (World Health Organization) Neurological DisordersDocument232 pages(World Health Organization) Neurological DisordersAlina BreazuNo ratings yet
- Johnny Be Good Tonight Updated PDFDocument120 pagesJohnny Be Good Tonight Updated PDFbodeadumitru9261No ratings yet
- Baltic Amber Handbook PDFDocument154 pagesBaltic Amber Handbook PDFbodeadumitru9261No ratings yet
- Tentorial IncisuraDocument23 pagesTentorial Incisurabodeadumitru9261100% (1)
- Cerebellum and Fourth VentricleDocument21 pagesCerebellum and Fourth Ventriclebodeadumitru9261100% (2)
- Products PDFs NeuroCriticalCare Camino BrochureDocument0 pagesProducts PDFs NeuroCriticalCare Camino Brochurebodeadumitru9261No ratings yet
- Autoimmune NeurologicalDocument385 pagesAutoimmune Neurologicalbodeadumitru9261No ratings yet
- Behavioral Management of Exercise Training in Vascular Headache Patients: An Investigation of Exercise Adherence and Headache ActivityDocument11 pagesBehavioral Management of Exercise Training in Vascular Headache Patients: An Investigation of Exercise Adherence and Headache Activitybodeadumitru9261No ratings yet
- Physical Exercise and PsychologicalDocument10 pagesPhysical Exercise and Psychologicalbodeadumitru9261100% (1)
- The Cerebellar ArteriesDocument40 pagesThe Cerebellar Arteriesbodeadumitru9261100% (1)
- Human Body EncyclopediaDocument124 pagesHuman Body EncyclopediaMaria TilvarNo ratings yet
- DukeDocument35 pagesDukebodeadumitru9261No ratings yet
- CNS LymphomasDocument8 pagesCNS Lymphomasbodeadumitru9261100% (1)
- Surgical Trial in Lobar Intracerebral Haemorrhage Protocol: Version 1.3 / 10 August 2006Document23 pagesSurgical Trial in Lobar Intracerebral Haemorrhage Protocol: Version 1.3 / 10 August 2006bodeadumitru9261100% (1)
- ATLASV2Document476 pagesATLASV2bodeadumitru9261100% (1)
- Full TextDocument9 pagesFull Textbodeadumitru9261No ratings yet
- CT ProtocolsDocument1 pageCT ProtocolsRaghad BabourNo ratings yet
- Principles of Anatomy and Physiology: 14th EditionDocument47 pagesPrinciples of Anatomy and Physiology: 14th EditionDayledaniel SorvetoNo ratings yet
- Shoulder Joint Complex - 1Document6 pagesShoulder Joint Complex - 1Alia ShabbirNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Principle Dentofacial OrthopedicsDocument10 pagesPrinciple Dentofacial Orthopedicsyuni madjidNo ratings yet
- PDF Marathon Legs 07.13.20Document2 pagesPDF Marathon Legs 07.13.20Alberto Sáez CastilloNo ratings yet
- Axial Skeletal SummaryDocument21 pagesAxial Skeletal SummaryBSMT 1-1, TAN, NICOLE SELINA L.No ratings yet
- Centric Relation and Centric OcclusionDocument3 pagesCentric Relation and Centric OcclusionYumi Sayade DentistryNo ratings yet
- Extremitas Radiography Interpretation: Faculty of Veterinary Medicine, IPB University Telp: +62 8111191333 (Abby Pratama)Document2 pagesExtremitas Radiography Interpretation: Faculty of Veterinary Medicine, IPB University Telp: +62 8111191333 (Abby Pratama)Intan PradikaNo ratings yet
- Biomechanics and Muscular-Activity During Sit-to-Stand TransferDocument11 pagesBiomechanics and Muscular-Activity During Sit-to-Stand TransferAh ZhangNo ratings yet
- DislocationDocument46 pagesDislocationShaa ShawalishaNo ratings yet
- Anatomi & Fisiologi IDocument25 pagesAnatomi & Fisiologi ISyasya NanaNo ratings yet
- Shoulder Boulder ExerciseDocument2 pagesShoulder Boulder Exerciseadityakavtiyal9No ratings yet
- LAS-in-PE-9-MARCH-6-7 QuaghDocument2 pagesLAS-in-PE-9-MARCH-6-7 QuaghJhunred AycochoNo ratings yet
- Titanium Elastic Nail PDFDocument27 pagesTitanium Elastic Nail PDFAmith AlankarNo ratings yet
- Saareera Marma Vignyanam PDFDocument53 pagesSaareera Marma Vignyanam PDFgandhiayuNo ratings yet
- Shoulder Exercise Descriptions For BankartDocument10 pagesShoulder Exercise Descriptions For BankartIlmuddin ApridhantikoNo ratings yet
- Rabbit (Oryctolagus Cuniculus) Muscular System: I. Dermal/IntegumentaryDocument9 pagesRabbit (Oryctolagus Cuniculus) Muscular System: I. Dermal/IntegumentaryAnnray Justine T. GlipaNo ratings yet
- Skeletal TractionDocument7 pagesSkeletal TractionAnnalyn Austria100% (2)
- DLP-PE-11 - Week 5Document5 pagesDLP-PE-11 - Week 5Jonalyn FacultadNo ratings yet
- LBPDocument27 pagesLBPAnonymous 7jKR9XbNo ratings yet
- Upper Body Exercises For Pitcher: by Chris Spielman, Instructor, Windmill Clinics, St. Charles, ILDocument2 pagesUpper Body Exercises For Pitcher: by Chris Spielman, Instructor, Windmill Clinics, St. Charles, ILJustin MillerNo ratings yet
- Nevralgia Cervico-BrahealaDocument17 pagesNevralgia Cervico-BrahealaAlex RăşcanuNo ratings yet
- Vicente Sanchis-Alfonso MD, PHD (Auth.), Stefano Zaffagnini, David Dejour, Elizabeth A. Arendt (Eds.) Patellofemoral Pain, Instability, and Arthritis - Clinical Presentation, Imaging, and Treatmen PDFDocument324 pagesVicente Sanchis-Alfonso MD, PHD (Auth.), Stefano Zaffagnini, David Dejour, Elizabeth A. Arendt (Eds.) Patellofemoral Pain, Instability, and Arthritis - Clinical Presentation, Imaging, and Treatmen PDFgoogleNo ratings yet
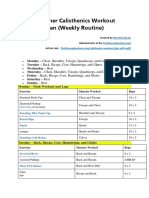
- Beginner Calisthenics Workout Routine PDFDocument3 pagesBeginner Calisthenics Workout Routine PDFGamer's PrideNo ratings yet