You might also like
- PNC Registration Form - 2Document2 pagesPNC Registration Form - 2umair J Abbasi71% (17)
- Computerised Payroll Practice Set Using MYOB AccountRight: Australian EditionFrom EverandComputerised Payroll Practice Set Using MYOB AccountRight: Australian EditionNo ratings yet
- Pakistan Nursing Council Pakistan Nursing Council Pakistan Nursing CouncilDocument2 pagesPakistan Nursing Council Pakistan Nursing Council Pakistan Nursing CouncilHameed Khan78% (9)
- Pakistan Nursing Council Pakistan Nursing Council Pakistan Nursing CouncilDocument2 pagesPakistan Nursing Council Pakistan Nursing Council Pakistan Nursing CouncilHameed Khan100% (2)
- Application Form - Non TeachingDocument7 pagesApplication Form - Non TeachinginglebymillNo ratings yet
- The British High Commission Is An Equal Opportunity EmployerDocument4 pagesThe British High Commission Is An Equal Opportunity EmployerFahim John BhattiNo ratings yet
- 10K Women Application Apr 2011 V2Document4 pages10K Women Application Apr 2011 V2Manjeet RathoreNo ratings yet
- Sikkim Public Service Commission: Application Form For The Post of Veterinary OfficerDocument4 pagesSikkim Public Service Commission: Application Form For The Post of Veterinary OfficerJeshiNo ratings yet
- Veiw Application FormDocument15 pagesVeiw Application FormKislay Rakesh ShahiNo ratings yet
- HR FormDocument4 pagesHR FormRawalpindi Arts CouncilNo ratings yet
- CSS Application FormDocument11 pagesCSS Application FormAltaf SheikhNo ratings yet
- 03 Pif PDFDocument11 pages03 Pif PDFPein NguyenNo ratings yet
- Annexure-I Bio-Data Form Advt - No.:BDL/C-P&A/PLG.&ED./2015-3: Page 1 of 4Document4 pagesAnnexure-I Bio-Data Form Advt - No.:BDL/C-P&A/PLG.&ED./2015-3: Page 1 of 4Venu KinngNo ratings yet
- BEML Limited: Application FormDocument10 pagesBEML Limited: Application FormJeshiNo ratings yet
- Sap Joining Form PRASHANTDocument4 pagesSap Joining Form PRASHANTOnkar ChavanNo ratings yet
- Application Form: Section 1 Personal DetailsDocument9 pagesApplication Form: Section 1 Personal DetailsLinh TranNo ratings yet
- Annexure-I Bio-Data Form Advt - No.:BDL/C-P&A/PLG.&ED./2012-5: Page 1 of 4Document4 pagesAnnexure-I Bio-Data Form Advt - No.:BDL/C-P&A/PLG.&ED./2012-5: Page 1 of 4Ramanareddy AnathapurNo ratings yet
- Annexure-I Bio-Data Form Advt - No.:BDL/C-P&A/PLG.&ED./2011-4: Page 1 of 4Document4 pagesAnnexure-I Bio-Data Form Advt - No.:BDL/C-P&A/PLG.&ED./2011-4: Page 1 of 4mauryaaarunNo ratings yet
- ITC ILO Turin Course - Application FormDocument6 pagesITC ILO Turin Course - Application FormMirza Muhammad Adnan0% (1)
- PWD fORMDocument4 pagesPWD fORMShahbaz ManzoorNo ratings yet
- Affix Self Attested Latest Color Photograph: Application Format For Recruitment ofDocument2 pagesAffix Self Attested Latest Color Photograph: Application Format For Recruitment ofVishal NarnauliaNo ratings yet
- New Grad Job AppDocument2 pagesNew Grad Job AppTanveer TanuNo ratings yet
- On-Line Application For Recruitment of Specialist OfficersDocument3 pagesOn-Line Application For Recruitment of Specialist OfficerssunittandonjNo ratings yet
- Udyami Application ProformaDocument3 pagesUdyami Application ProformaTanuj KujurNo ratings yet
- Singaporean/Malaysian Cabin Crew Application FormDocument2 pagesSingaporean/Malaysian Cabin Crew Application FormLuvjot Tan SinghNo ratings yet
- Enrolment Form AadharDocument2 pagesEnrolment Form AadhardrmohangNo ratings yet
- COB Employment Application Revised 2016Document5 pagesCOB Employment Application Revised 2016Anonymous 78HlUFaWNo ratings yet
- Indian Institute of Technology PatnaDocument6 pagesIndian Institute of Technology PatnaSaurabh ChhabraNo ratings yet
- Biocon ApplicationDocument5 pagesBiocon ApplicationGururaj NadagerNo ratings yet
- On-Line Application For Recruitment of Apprentice Development Officers-2012-13Document3 pagesOn-Line Application For Recruitment of Apprentice Development Officers-2012-13Charles Darvin ThirunavukkarsuNo ratings yet
- OPF Job Application FormDocument1 pageOPF Job Application FormAbdul WadoodNo ratings yet
- Job Application FormDocument3 pagesJob Application FormSchakema Mohamad100% (1)
- Bimk-Kadapa: Application FormDocument2 pagesBimk-Kadapa: Application FormPrashanthNo ratings yet
- Application Cum Personal Data FormDocument5 pagesApplication Cum Personal Data Formsunil_rkzNo ratings yet
- ICAP Form A ApplicationDocument2 pagesICAP Form A ApplicationBASEER AHMEDNo ratings yet
- Apply for Top MBA ProgramsDocument7 pagesApply for Top MBA ProgramsRemisha MaharjanNo ratings yet
- Application For EmploymentDocument4 pagesApplication For EmploymentVanshbabbarNo ratings yet
- Disney India background verification formDocument7 pagesDisney India background verification formSameer ParabNo ratings yet
- Employment Application 1Document4 pagesEmployment Application 1zaininfo786No ratings yet
- Standard Application Format Aa India Jobs Aug 2012Document5 pagesStandard Application Format Aa India Jobs Aug 2012Thangaraj MswNo ratings yet
- Revised Attestation FormDocument15 pagesRevised Attestation Formk.nagendraraoNo ratings yet
- ProjectDocument2 pagesProjectDebankan ChakrabortyNo ratings yet
- Request Form For Reference LetterDocument2 pagesRequest Form For Reference LetterVIRTUAL UNIVERSITYNo ratings yet
- Wapcos FormDocument2 pagesWapcos FormyagrashokNo ratings yet
- WAPCOS LTD. BIO DATADocument2 pagesWAPCOS LTD. BIO DATAAjay PrajapatiNo ratings yet
- Employment - Form NetsolDocument8 pagesEmployment - Form Netsol9874567No ratings yet
- Enrolment FormDocument2 pagesEnrolment Formapi-291451017No ratings yet
- Registered Nurses Philippines Health Service ApplicationDocument1 pageRegistered Nurses Philippines Health Service ApplicationNica NixNo ratings yet
- BRITISH DEPUTY HIGH COMMISSION JOB APPLICATIONDocument4 pagesBRITISH DEPUTY HIGH COMMISSION JOB APPLICATIONmalikshafiq_1No ratings yet
- Application For Employment: in ConfidenceDocument6 pagesApplication For Employment: in ConfidenceGlenn Bede A.BenabloNo ratings yet
- Employment Form NewDocument8 pagesEmployment Form Newsunru24No ratings yet
- Apply for Newport City Council positionDocument6 pagesApply for Newport City Council positionuonwNo ratings yet
- Credit Card Application Public Supplementary SaveableDocument2 pagesCredit Card Application Public Supplementary Saveablemcad_marieNo ratings yet
- S T NS T N District & Sessions Court Bahawalnagar: Recruitment TestDocument4 pagesS T NS T N District & Sessions Court Bahawalnagar: Recruitment TestMaqsood JavaidNo ratings yet
- Affix Your Recent Passport Size Photograph Here: Application FormatDocument1 pageAffix Your Recent Passport Size Photograph Here: Application FormatGurubasavaraju T MNo ratings yet
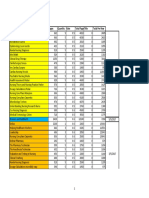
- Book Name Pages Quantity Rate Total Pagestitle Total Per RowDocument3 pagesBook Name Pages Quantity Rate Total Pagestitle Total Per RowRaheelNo ratings yet
- Qlinks A&b and Shoby CV 6 1Document3 pagesQlinks A&b and Shoby CV 6 1RaheelNo ratings yet
- Essentials of Pharmacology For NursesDocument2 pagesEssentials of Pharmacology For NursesRaheelNo ratings yet
- Bug List Setup PageDocument2 pagesBug List Setup PageRaheelNo ratings yet
- CV Fatima Kamal Seeking Career with Progressive CompanyDocument1 pageCV Fatima Kamal Seeking Career with Progressive CompanyRaheelNo ratings yet
- Wedding CardDocument1 pageWedding CardRaheelNo ratings yet
- Bhand ListDocument2 pagesBhand ListRaheelNo ratings yet
- Tetanus Prophylaxis in Wounds - UKDocument1 pageTetanus Prophylaxis in Wounds - UKRaheelNo ratings yet
- Database AnalysisDocument4 pagesDatabase AnalysisRaheelNo ratings yet
- 9999 SundayDocument1 page9999 SundayRaheelNo ratings yet
- Daily TitlesDocument6 pagesDaily TitlesRaheelNo ratings yet
- RaheelDocument2 pagesRaheelRaheelNo ratings yet
- QA Basic Check ListDocument1 pageQA Basic Check ListRaheelNo ratings yet
- Flat No B204 Green Garden, Garden West Karachi: Helix Publilsher Bill ToDocument1 pageFlat No B204 Green Garden, Garden West Karachi: Helix Publilsher Bill ToRaheelNo ratings yet
- New Books & Books Purchase Order: Code Product Name Qty (L) Amount Cost Price Pack Qty (P)Document1 pageNew Books & Books Purchase Order: Code Product Name Qty (L) Amount Cost Price Pack Qty (P)RaheelNo ratings yet
- New Books & Books, Multan PO 3 for Helix PublisherDocument3 pagesNew Books & Books, Multan PO 3 for Helix PublisherRaheelNo ratings yet
- Flat No B204 Green Garden, Garden West Karachi: Helix Publilsher Bill ToDocument2 pagesFlat No B204 Green Garden, Garden West Karachi: Helix Publilsher Bill ToRaheelNo ratings yet
- New Books & Books Purchase Order: PO PO Date Vendor Name Address Description Print Date: Print TimeDocument2 pagesNew Books & Books Purchase Order: PO PO Date Vendor Name Address Description Print Date: Print TimeRaheelNo ratings yet
- New Books & Books Purchase Order: PO PO Date Vendor Name Address Description Print Date: Print TimeDocument3 pagesNew Books & Books Purchase Order: PO PO Date Vendor Name Address Description Print Date: Print TimeRaheelNo ratings yet
- Invoice for Photocopy Printing for Idrees MultanDocument1 pageInvoice for Photocopy Printing for Idrees MultanRaheelNo ratings yet
- Daily TitlesDocument2 pagesDaily TitlesRaheelNo ratings yet
- Cpry Item Id Author Title ED Stock Status Local Pub DateDocument11 pagesCpry Item Id Author Title ED Stock Status Local Pub DateRaheelNo ratings yet
- HelixDocument1 pageHelixRaheelNo ratings yet
- Purchase Order: Order ID: 23 Helix Publilsher Vednor: DateDocument1 pagePurchase Order: Order ID: 23 Helix Publilsher Vednor: DateRaheelNo ratings yet
- RCEM Curriculum 05 03 15 For August 2015 FINAL AMENDED 05 06 15 .PDF 61270597Document392 pagesRCEM Curriculum 05 03 15 For August 2015 FINAL AMENDED 05 06 15 .PDF 61270597RaheelNo ratings yet
- Product/Service Description Unit Cost Quantity Discount PriceDocument1 pageProduct/Service Description Unit Cost Quantity Discount PriceRaheelNo ratings yet
- New Books & Books Purchase Order for Helix PublisherDocument2 pagesNew Books & Books Purchase Order for Helix PublisherRaheelNo ratings yet
- New Books & Books Purchase Order for Helix PublisherDocument2 pagesNew Books & Books Purchase Order for Helix PublisherRaheelNo ratings yet
- DDDDDDocument24 pagesDDDDDRaheelNo ratings yet
- Delivering Policy Reform: Anchoring Significant Reforms in Turbulent TimesDocument230 pagesDelivering Policy Reform: Anchoring Significant Reforms in Turbulent TimesRaheelNo ratings yet
- Final Educ 8Document40 pagesFinal Educ 8Ive EspiaNo ratings yet
- Progress Report 1 - Olivia Day - s5056250Document19 pagesProgress Report 1 - Olivia Day - s5056250api-375225559No ratings yet
- JEE Advanced SolutionsDocument11 pagesJEE Advanced SolutionsshreyashNo ratings yet
- Introduction To Modern Political Thought PDFDocument48 pagesIntroduction To Modern Political Thought PDFbijonhazarika50% (2)
- Philippine Constitution provisions on educationDocument2 pagesPhilippine Constitution provisions on educationLouise salesNo ratings yet
- The City Boundary in Late Antique RomeDocument308 pagesThe City Boundary in Late Antique RomeJoshua Immanuel GaniNo ratings yet
- 2023 New Intakes Acceptance ListDocument33 pages2023 New Intakes Acceptance Listezekiel leoNo ratings yet
- Employment Transition of Fresh Business Graduates An AssessmentDocument49 pagesEmployment Transition of Fresh Business Graduates An AssessmentCyan Vincent CanlasNo ratings yet
- Really Great Reading Diagnostic Decoding SurveysDocument20 pagesReally Great Reading Diagnostic Decoding Surveysapi-331571310100% (1)
- Hifz QuranDocument3 pagesHifz QuranikamableNo ratings yet
- ValueDocument4 pagesValueAshpreetNo ratings yet
- Training Design & Matrix-DapsshiDocument11 pagesTraining Design & Matrix-Dapsshimharlit cagaananNo ratings yet
- Rifky Wisnuardi Waskito - B0901201075 - MK Kesrawan - Sapi PerahDocument9 pagesRifky Wisnuardi Waskito - B0901201075 - MK Kesrawan - Sapi Perahrifky waskitoNo ratings yet
- BET 2101 - Lesson 3-Peer Teaching and Media PracticalsDocument26 pagesBET 2101 - Lesson 3-Peer Teaching and Media PracticalsElija ChesainaNo ratings yet
- Nurse LifeDocument9 pagesNurse Lifeapi-310647920100% (1)
- Grade 12 - Class Program 2023-2024Document2 pagesGrade 12 - Class Program 2023-2024Rovelyn ClementeNo ratings yet
- Resume UpdatedDocument6 pagesResume UpdatedBryan Romena EvangelistaNo ratings yet
- Tyler Junior College Catalog 2022-2023 - CopieDocument289 pagesTyler Junior College Catalog 2022-2023 - Copieغير نفسكNo ratings yet
- Literature ModuleDocument4 pagesLiterature ModuleShawn Michael PeraterNo ratings yet
- Lesson Plan On Earth and Life Science 11, Midterm Module 3: Natural Hazards, Mitigation and AdaptationDocument8 pagesLesson Plan On Earth and Life Science 11, Midterm Module 3: Natural Hazards, Mitigation and AdaptationAlthea VargasNo ratings yet
- Catcher in The Rye EssayDocument2 pagesCatcher in The Rye Essayapi-269595464No ratings yet
- ANHS Senior High School Class ProgramDocument4 pagesANHS Senior High School Class Programapi-450904901No ratings yet
- Intro to Native American Social PsychDocument7 pagesIntro to Native American Social PsychCj IsoNo ratings yet
- Winners Don't Do Different Things - They Do Things Differently .......Document14 pagesWinners Don't Do Different Things - They Do Things Differently .......Manvi Gupta100% (1)
- New Product DevelopmentDocument41 pagesNew Product DevelopmentYodhia Antariksa96% (24)
- CV and Covering Letter Worksheet - Tourism IVDocument2 pagesCV and Covering Letter Worksheet - Tourism IVJonatan Gárate Aros HofstadterNo ratings yet
- Nail Care Lesson PlanDocument4 pagesNail Care Lesson PlanNhil Cabillon QuietaNo ratings yet
- FetchDocument11 pagesFetchMargarida FerreiraNo ratings yet
- BioMedicine - I3lDocument6 pagesBioMedicine - I3lAhmad AnshaveforeverNo ratings yet