You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Your New Bill.: 30 October 2020Document4 pagesYour New Bill.: 30 October 2020Юлия П75% (4)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Robert VenturiDocument28 pagesRobert VenturiPankaj Dhaked100% (1)
- Deputy General Manager Duties and ResponsibilitiesDocument6 pagesDeputy General Manager Duties and Responsibilitiesstanis555No ratings yet
- Deputy General Manager Duties and ResponsibilitiesDocument3 pagesDeputy General Manager Duties and Responsibilitiesstanis555No ratings yet
- CC ExcutiveDocument2 pagesCC Excutivestanis555No ratings yet
- Chief Medical Officer Job Duties: Required Knowledge, Skills and AbilitiesDocument2 pagesChief Medical Officer Job Duties: Required Knowledge, Skills and Abilitiesstanis555100% (1)
- Duty DoctorDocument1 pageDuty Doctorstanis555No ratings yet
- Infra in ICUDocument1 pageInfra in ICUstanis555No ratings yet
- Projects Questions To AskedDocument6 pagesProjects Questions To Askedstanis555No ratings yet
- Part B Intensive Care UnitDocument10 pagesPart B Intensive Care Unitstanis555No ratings yet
- NOC Fire and SaftyDocument2 pagesNOC Fire and Saftystanis555No ratings yet
- StagesDocument1 pageStagesstanis555No ratings yet
- Engineering ServicesDocument1 pageEngineering Servicesstanis555No ratings yet
- Requirement HospitalDocument1 pageRequirement Hospitalstanis555No ratings yet
- Kpme Application Details RequiredDocument2 pagesKpme Application Details Requiredstanis555No ratings yet
- Feasibility StudyDocument4 pagesFeasibility Studystanis555No ratings yet
- TechnoFunda Investing Screener Excel Template - VFDocument27 pagesTechnoFunda Investing Screener Excel Template - VFstanis555No ratings yet
- Iimk SMPHC BrochureDocument17 pagesIimk SMPHC Brochurestanis555No ratings yet
- Stages of Hospital DevelopmentDocument16 pagesStages of Hospital Developmentstanis555100% (1)
- Hospital MapDocument1 pageHospital Mapstanis555No ratings yet
- Suture Materials & TechniquesDocument31 pagesSuture Materials & Techniquesstanis555100% (6)
- Pre OperativeDocument5 pagesPre Operativestanis555100% (1)
- Unit 1Document59 pagesUnit 1ayush charde 786No ratings yet
- Impact of Climate Change On Floriculture and Landscape GardeningDocument38 pagesImpact of Climate Change On Floriculture and Landscape GardeningRuby SarmahNo ratings yet
- Marketing Plan - MattDocument22 pagesMarketing Plan - MattMatt ENo ratings yet
- Introduction To Reverse Engineering: October 2007Document10 pagesIntroduction To Reverse Engineering: October 2007Sudeep Kumar Singh100% (1)
- Libor Market Model Specification and CalibrationDocument29 pagesLibor Market Model Specification and CalibrationGeorge LiuNo ratings yet
- Gas Power CycleDocument42 pagesGas Power CycleAdrianNo ratings yet
- WB - Soft Drinks in 2021 - New WellbeingDocument18 pagesWB - Soft Drinks in 2021 - New WellbeingalexmgbNo ratings yet
- MANUALESDocument84 pagesMANUALESPedroJose0% (1)
- Effective MFA For PeopleSoft DataSheet Appsian 2020Document2 pagesEffective MFA For PeopleSoft DataSheet Appsian 2020pnorbertoNo ratings yet
- IDFT & CONVOLUTIONS - PROBLEMS Part 6Document19 pagesIDFT & CONVOLUTIONS - PROBLEMS Part 6Abishek RajeshNo ratings yet
- Textbook Prism and Lens Making A Textbook For Optical Glassworkers Second Edition Frank Twyman Ebook All Chapter PDFDocument53 pagesTextbook Prism and Lens Making A Textbook For Optical Glassworkers Second Edition Frank Twyman Ebook All Chapter PDFleon.beattie194100% (5)
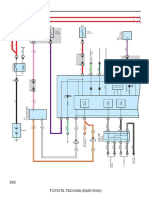
- Combination Meter: 262 Toyota Tacoma (Em01D0U)Document6 pagesCombination Meter: 262 Toyota Tacoma (Em01D0U)hamayunNo ratings yet
- Product Sheet: Heat Transfer FluidsDocument21 pagesProduct Sheet: Heat Transfer FluidsjeyderNo ratings yet
- RoboticsbasicDocument52 pagesRoboticsbasicdanvicNo ratings yet
- Research Paper On Purity and Its Importance in Islam and Among MuslimsDocument18 pagesResearch Paper On Purity and Its Importance in Islam and Among MuslimsSadia SiddiquiNo ratings yet
- Re - Meteorological Data CostDocument2 pagesRe - Meteorological Data CostJahanzeb KhanNo ratings yet
- MRC Pylon Racer PDFDocument16 pagesMRC Pylon Racer PDF3 studsNo ratings yet
- L4 - Structure of Metals - EMPDocument8 pagesL4 - Structure of Metals - EMPkopkash123No ratings yet
- Luis J Corona ResumeDocument2 pagesLuis J Corona Resumeapi-337110849No ratings yet
- No More NegativityDocument11 pagesNo More NegativityIoana PaulNo ratings yet
- Atex Directive in A NutshellDocument4 pagesAtex Directive in A NutshellAnonymous 96SYLheENo ratings yet
- Generator Breaker Equipped With Vacuum InterruptersDocument4 pagesGenerator Breaker Equipped With Vacuum InterruptersVenna Karthik ReddyNo ratings yet
- PL2303 G Series ManualDocument1 pagePL2303 G Series ManualGesiNo ratings yet
- Clause - 1 FansDocument441 pagesClause - 1 Fansvel mech100% (1)
- Cases Histories and Recent Development of The Sand Compaction PilDocument7 pagesCases Histories and Recent Development of The Sand Compaction PilVetriselvan ArumugamNo ratings yet
- Lecture-1 Introduction To Power Generation and Electrical Power SystemsDocument30 pagesLecture-1 Introduction To Power Generation and Electrical Power SystemsArishaNo ratings yet
- Mobile COMPUTINGDocument169 pagesMobile COMPUTINGNPMYS23No ratings yet
- Horn AntennasDocument29 pagesHorn AntennasAbderrahmane BadisNo ratings yet