You might also like
- Infections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumFrom EverandInfections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumNo ratings yet
- Rev 5 NeutroDocument10 pagesRev 5 Neutroapi-255084253No ratings yet
- Histopathology Reporting: Guidelines for Surgical CancerFrom EverandHistopathology Reporting: Guidelines for Surgical CancerDavid P. BoyleNo ratings yet
- Rev 3 NeutropolicyDocument11 pagesRev 3 Neutropolicyapi-255084253No ratings yet
- Rev 1 NeutroDocument9 pagesRev 1 Neutroapi-255084253No ratings yet
- Rev 9 NeutroDocument10 pagesRev 9 Neutroapi-255084253No ratings yet
- BarbsrevisionsnpDocument9 pagesBarbsrevisionsnpapi-255084253No ratings yet
- Infections in Surgery: Prevention and ManagementFrom EverandInfections in Surgery: Prevention and ManagementMassimo SartelliNo ratings yet
- NeutrotoppppcDocument10 pagesNeutrotoppppcapi-255084253No ratings yet
- Philippine Guidelines on Diagnosis and Management of CAPDocument13 pagesPhilippine Guidelines on Diagnosis and Management of CAPRaine CentinoNo ratings yet
- Diagnostic Approach To The Adult Presenting With Neutropenic FeverDocument7 pagesDiagnostic Approach To The Adult Presenting With Neutropenic FeverAseret IlecaraNo ratings yet
- Anderson01-27-12 Floroquinolone Prophilaxis PDFDocument22 pagesAnderson01-27-12 Floroquinolone Prophilaxis PDFSri WulandahNo ratings yet
- Treatment of Neutropenic Fever Syndromes in Adults With Hematologic Malignancies and Hematopoietic CDocument20 pagesTreatment of Neutropenic Fever Syndromes in Adults With Hematologic Malignancies and Hematopoietic CAseret IlecaraNo ratings yet
- ABSTRACT: Cancer Patients Who Develop Infections, Especially Those Receiving ChemotherapyDocument5 pagesABSTRACT: Cancer Patients Who Develop Infections, Especially Those Receiving Chemotherapygod4alllNo ratings yet
- FN 2011 IdsaDocument38 pagesFN 2011 IdsaNuttawath UngwichanpunyaNo ratings yet
- Clinical Practice Guideline For The Use of Antimicrobial Agents in Nutropenic Patients CID 11Document38 pagesClinical Practice Guideline For The Use of Antimicrobial Agents in Nutropenic Patients CID 11Mariela ColomboNo ratings yet
- Managing Hemato Oncology Patients in EdDocument6 pagesManaging Hemato Oncology Patients in EdjprakashjjNo ratings yet
- Necrotizing Pneumonia in Cancer Patients A.8Document4 pagesNecrotizing Pneumonia in Cancer Patients A.8Manisha UppalNo ratings yet
- 10 5811@westjem 2018 12 37335Document8 pages10 5811@westjem 2018 12 37335bobNo ratings yet
- Pneumonia: V. Mandang, M.DDocument44 pagesPneumonia: V. Mandang, M.DMeggy SumarnoNo ratings yet
- Selected Oncologic Emergencies: Sandra S. Ugras-ReyDocument13 pagesSelected Oncologic Emergencies: Sandra S. Ugras-ReyJustene PeñamoraNo ratings yet
- Febrile NeutropeniaDocument35 pagesFebrile NeutropeniaYogesh ShindeNo ratings yet
- 08 Pneumonia Review ofDocument4 pages08 Pneumonia Review ofMonika Margareta Maria ElviraNo ratings yet
- Nosocomial Pneumonia: Self AssessmentDocument10 pagesNosocomial Pneumonia: Self AssessmentZali AhmadNo ratings yet
- Diagnosis and Management of Febrile Neutropenia 4567Document6 pagesDiagnosis and Management of Febrile Neutropenia 4567Hisham ElhadidiNo ratings yet
- LOW PLT THRESHOLD GUIDELINESDocument13 pagesLOW PLT THRESHOLD GUIDELINESBill Alfred LaporeNo ratings yet
- Febrile Neutropenia PublishedDocument6 pagesFebrile Neutropenia PublishedahmadheulwanNo ratings yet
- Overview of Neutropenic Fever SyndromesDocument16 pagesOverview of Neutropenic Fever Syndromesnon_zenseNo ratings yet
- Clinical Practice Guideline For The Use of Antimicrobial Agents in Neutropenic Patients With CancerDocument38 pagesClinical Practice Guideline For The Use of Antimicrobial Agents in Neutropenic Patients With CancerAini Sofa HaniahNo ratings yet
- Journal Reading Tonsilitis Akut PDFDocument6 pagesJournal Reading Tonsilitis Akut PDFTaufiq HidayatNo ratings yet
- PCP Pneumonia GuideDocument15 pagesPCP Pneumonia GuideMuzyone WanNo ratings yet
- 05 Investigations For PneumoniaDocument4 pages05 Investigations For Pneumoniause4meNo ratings yet
- Clinical OncologyDocument8 pagesClinical OncologyHector VillaseñorNo ratings yet
- tmpC1E4 TMPDocument6 pagestmpC1E4 TMPFrontiersNo ratings yet
- ShuntDocument13 pagesShuntVijayakanth VijayakumarNo ratings yet
- Nursing Care Plan: Nursing Diagnosis Analysis Goal and Objectives Nursing Interventions Rationale EvaluationDocument3 pagesNursing Care Plan: Nursing Diagnosis Analysis Goal and Objectives Nursing Interventions Rationale EvaluationPaul Cubacub100% (1)
- 2014 Article 639Document8 pages2014 Article 639Anida HasnaNo ratings yet
- Antibiotice in Terapie IntensivaDocument9 pagesAntibiotice in Terapie IntensivaLiliana NăstaseNo ratings yet
- Enteric Fever (Typhoid and Paratyphoid) in Adult Treatment Guidelines (UHL)Document3 pagesEnteric Fever (Typhoid and Paratyphoid) in Adult Treatment Guidelines (UHL)fildzah amalyaNo ratings yet
- Guidelines for HAP and VAP ManagementDocument43 pagesGuidelines for HAP and VAP ManagementSarah Ummah MNo ratings yet
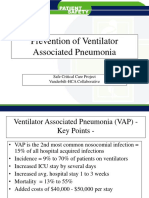
- Prevention of Ventilator Associated Pneumonia: Safe Critical Care Project Vanderbilt-HCA CollaborativeDocument21 pagesPrevention of Ventilator Associated Pneumonia: Safe Critical Care Project Vanderbilt-HCA CollaborativeapipNo ratings yet
- Febrile Neutropenia UptodateDocument25 pagesFebrile Neutropenia UptodateMayar MoustafaNo ratings yet
- 0221 Community-Acquired-PneumoniaDocument29 pages0221 Community-Acquired-PneumoniaDiego YanezNo ratings yet
- Non-Tuberculous Mycobacterial Pulmonary Infections: ReviewDocument12 pagesNon-Tuberculous Mycobacterial Pulmonary Infections: Reviewmgoez077No ratings yet
- Infection in CancerDocument34 pagesInfection in CancerSheikNo ratings yet
- Neutropenic Fever Empiric TherapyDocument5 pagesNeutropenic Fever Empiric TherapyRominaPulvermüllerSalvatierraNo ratings yet
- Neutropenic SepsisDocument38 pagesNeutropenic SepsisYS NateNo ratings yet
- Emergency MedDocument4 pagesEmergency MedbencleeseNo ratings yet
- Rheumatic Heart DiseasesDocument21 pagesRheumatic Heart DiseasesMuna Hassan MustafaNo ratings yet
- Multidisciplinary Case-Based Teaching: Prof. S. O 'Neill Dr. D. Royston Dr. S. ShaikhDocument90 pagesMultidisciplinary Case-Based Teaching: Prof. S. O 'Neill Dr. D. Royston Dr. S. Shaikhmynoidanh19No ratings yet
- Oncologic EmergenciesDocument32 pagesOncologic EmergenciesColleen BernilNo ratings yet
- The Incidence of Thrombophlebitis Following The Use of Peripheral Intravenous Cannula in Post-Operative Patients A Prospective Observational StudyDocument4 pagesThe Incidence of Thrombophlebitis Following The Use of Peripheral Intravenous Cannula in Post-Operative Patients A Prospective Observational StudyIOSRjournalNo ratings yet
- Use of F-FDG PET To Predict Response To First-Line Tuberculostatics in HIV-Associated TuberculosisDocument6 pagesUse of F-FDG PET To Predict Response To First-Line Tuberculostatics in HIV-Associated TuberculosisdhaniNo ratings yet
- Antibiotics 02 00001Document10 pagesAntibiotics 02 00001Jenny AlmagroNo ratings yet
- COVIDDocument9 pagesCOVIDryan smithNo ratings yet
- Severe Systemic Cytomegalovirus Infection in An Immunocompetent Patient Outside The Intensive Care Unit: A Case ReportDocument4 pagesSevere Systemic Cytomegalovirus Infection in An Immunocompetent Patient Outside The Intensive Care Unit: A Case ReportSebastián Garay HuertasNo ratings yet
- Recurrent Respiratory Papillomatosis (RRP) : Basic Science To Clinical StudiesDocument16 pagesRecurrent Respiratory Papillomatosis (RRP) : Basic Science To Clinical StudiesLaura PayneNo ratings yet
- Final For GuidelinecomDocument10 pagesFinal For Guidelinecomapi-255084253No ratings yet
- NeutrotoppppcDocument10 pagesNeutrotoppppcapi-255084253No ratings yet
- OriginalneutropolicyDocument9 pagesOriginalneutropolicyapi-255084253No ratings yet
- Cna AcpcounciltemplateaprilDocument1 pageCna Acpcounciltemplateaprilapi-255084253No ratings yet
- Kyles Email Precepting AttendanceDocument2 pagesKyles Email Precepting Attendanceapi-255084253No ratings yet
- Cna AcpcounciltemplatefebDocument1 pageCna Acpcounciltemplatefebapi-255084253No ratings yet
- Summary Email of April MeetingsDocument2 pagesSummary Email of April Meetingsapi-255084253No ratings yet
- Advisor ChecklistDocument6 pagesAdvisor Checklistapi-255084253No ratings yet
- Cna FlyerDocument1 pageCna Flyerapi-255084253No ratings yet
- Cnaacuitytool 3Document1 pageCnaacuitytool 3api-255084253No ratings yet
- Cna AcpcounciltemplatemarchDocument1 pageCna Acpcounciltemplatemarchapi-255084253No ratings yet
- Email To Cnaacps About How To Access SPDocument1 pageEmail To Cnaacps About How To Access SPapi-255084253No ratings yet
- Minutes From 2-14 MeetingDocument4 pagesMinutes From 2-14 Meetingapi-255084253No ratings yet
- Pdca 2Document7 pagesPdca 2api-255084253No ratings yet
- Meeting Minutes From March EmailDocument1 pageMeeting Minutes From March Emailapi-255084253No ratings yet
- Mandatory April Meeting EmailDocument1 pageMandatory April Meeting Emailapi-255084253No ratings yet
- Minutes From 3-14 MeetingDocument2 pagesMinutes From 3-14 Meetingapi-255084253No ratings yet
- Email Confirmation From Anita All Cnas Are AddedDocument2 pagesEmail Confirmation From Anita All Cnas Are Addedapi-255084253No ratings yet
- Annsleys Response To FallsDocument2 pagesAnnsleys Response To Fallsapi-255084253No ratings yet
- Falls Question CnaacpsDocument2 pagesFalls Question Cnaacpsapi-255084253No ratings yet
- Precept Form From KaylaDocument3 pagesPrecept Form From Kaylaapi-255084253No ratings yet
- Email To Anita About SPDocument1 pageEmail To Anita About SPapi-255084253No ratings yet
- Sharepoint Vs Staff MeetingsDocument2 pagesSharepoint Vs Staff Meetingsapi-255084253No ratings yet
- Feedback Barb From Focus PdcaDocument2 pagesFeedback Barb From Focus Pdcaapi-255084253No ratings yet
- 1st Sharepoint Posting CnaDocument2 pages1st Sharepoint Posting Cnaapi-255084253No ratings yet
- Post Survey Respondent Unmatched Demographics UnmatchedDocument1 pagePost Survey Respondent Unmatched Demographics Unmatchedapi-255084253No ratings yet
- Email About Sharepoint and TitlingDocument1 pageEmail About Sharepoint and Titlingapi-255084253No ratings yet
- 5314 Look Report Cna EmailDocument2 pages5314 Look Report Cna Emailapi-255084253No ratings yet
- Post Survey Table MatchedDocument1 pagePost Survey Table Matchedapi-255084253No ratings yet
- Kayla Eval On MeDocument1 pageKayla Eval On Meapi-255084253No ratings yet
- Acute Suppurative Otitis MediaDocument41 pagesAcute Suppurative Otitis Mediarani suwadjiNo ratings yet
- Introduction To ParasitologyDocument6 pagesIntroduction To ParasitologyJoyce LeeNo ratings yet
- UTI antimicrobial formularyDocument109 pagesUTI antimicrobial formularySirawit Namkaeng ChoksuchatNo ratings yet
- 109 New Charm, CharmaidDocument2 pages109 New Charm, CharmaidAmit Kumar PandeyNo ratings yet
- Tips for Raising Laying Hens and Dairy CattleDocument12 pagesTips for Raising Laying Hens and Dairy CattleFerta Jaya SaputraNo ratings yet
- EPIDIOMOLOGYDocument8 pagesEPIDIOMOLOGYRose Anne AbivaNo ratings yet
- Visceral Leishmaniasis in IndiaDocument27 pagesVisceral Leishmaniasis in IndiaNishant SrivastavaNo ratings yet
- Introduction To Public HealthDocument24 pagesIntroduction To Public HealthGaurav PuriNo ratings yet
- Neonatal SepsisDocument6 pagesNeonatal SepsisSunaina AdhikariNo ratings yet
- Experiences of Students During The COVID-19 PandemicDocument7 pagesExperiences of Students During The COVID-19 Pandemiclovi poe100% (1)
- Dr. Huda R. Sabbar Al-Anbar University College of Medicine: HaemoflagellatesDocument19 pagesDr. Huda R. Sabbar Al-Anbar University College of Medicine: HaemoflagellatesThunderNo ratings yet
- Trematodes - Schistosomiasis (Asturias, Junsay)Document12 pagesTrematodes - Schistosomiasis (Asturias, Junsay)nnnnNo ratings yet
- UNIT 3 Biomedical Foundations of Public HealthDocument109 pagesUNIT 3 Biomedical Foundations of Public Healthgammaglutamyl dehydrogenaseNo ratings yet
- chn2 Lec ReviewerDocument11 pageschn2 Lec Reviewerella retizaNo ratings yet
- Pandemic Continuity of Operations PlanDocument14 pagesPandemic Continuity of Operations PlanAnalyn CanlasNo ratings yet
- Communicable Disease 2Document82 pagesCommunicable Disease 2pauline mangadaNo ratings yet
- India's Fight With Covid-Second WaveDocument1 pageIndia's Fight With Covid-Second WaveshwetaNo ratings yet
- Guillain Barre SyndromeDocument3 pagesGuillain Barre SyndromesohriaameroldimaporoNo ratings yet
- New COVID-19 entry protocols for FilipinosDocument5 pagesNew COVID-19 entry protocols for FilipinosmonchanNo ratings yet
- Comprehensive Review for Saudi Licence Exam for General DentistDocument4 pagesComprehensive Review for Saudi Licence Exam for General Dentistzoaib aliNo ratings yet
- Isolation and Identification of Bacteria From Lake Water in and Around Ranipet Area, Vellore DistrictDocument4 pagesIsolation and Identification of Bacteria From Lake Water in and Around Ranipet Area, Vellore DistrictDebjyotiDawnNo ratings yet
- A-2008 7th Semester International Humanitarian LawDocument24 pagesA-2008 7th Semester International Humanitarian LawSUYASH VISHWAKARMANo ratings yet
- Japanese Encephalitis Di Indonesia - JurnalDocument9 pagesJapanese Encephalitis Di Indonesia - JurnalMisyahHamisahSha'syahNo ratings yet
- BOOK - Advanced Pathology and Treatment of Diseases of Domestic Animals With Special Reference To Etiology, Signs, Pathology and Management 2008Document517 pagesBOOK - Advanced Pathology and Treatment of Diseases of Domestic Animals With Special Reference To Etiology, Signs, Pathology and Management 2008lumos_vnNo ratings yet
- Justification - PataganDocument15 pagesJustification - PataganMariroseNo ratings yet
- v170 v174 v175 Flockscreen Ai Instruction For Use v1Document7 pagesv170 v174 v175 Flockscreen Ai Instruction For Use v1Nader SedighiNo ratings yet
- BLA CK DEA TH: Spanis H FluDocument24 pagesBLA CK DEA TH: Spanis H FluShiela FranciscoNo ratings yet
- Virology AssignmentDocument7 pagesVirology AssignmentChethu ChethzNo ratings yet
- RITMDocument8 pagesRITMFrancineAntoinetteGonzalesNo ratings yet
- Bowel Nosodes Notes: Henry C Allen - Timing of Bowel Nosode RXDocument21 pagesBowel Nosodes Notes: Henry C Allen - Timing of Bowel Nosode RXFuente DelavidaNo ratings yet
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (5)
- The HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedFrom EverandThe HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedRating: 4.5 out of 5 stars4.5/5 (13)
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeFrom EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNo ratings yet
- The Price of Health: The Modern Pharmaceutical Industry and the Betrayal of a History of CareFrom EverandThe Price of Health: The Modern Pharmaceutical Industry and the Betrayal of a History of CareRating: 4.5 out of 5 stars4.5/5 (3)
- Coronary: A True Story of Medicine Gone AwryFrom EverandCoronary: A True Story of Medicine Gone AwryRating: 5 out of 5 stars5/5 (4)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyFrom EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyRating: 4 out of 5 stars4/5 (18)
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- The Invisible Rainbow: A History of Electricity and LifeFrom EverandThe Invisible Rainbow: A History of Electricity and LifeRating: 4.5 out of 5 stars4.5/5 (21)
- Epidemics and Society: From the Black Death to the PresentFrom EverandEpidemics and Society: From the Black Death to the PresentRating: 4.5 out of 5 stars4.5/5 (9)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (15)
- Arthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefFrom EverandArthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefNo ratings yet
- The Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceFrom EverandThe Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceNo ratings yet
- The Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeFrom EverandThe Hair Color Mix Book: More Than 150 Recipes for Salon-Perfect Color at HomeRating: 3.5 out of 5 stars3.5/5 (7)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanFrom EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanRating: 4.5 out of 5 stars4.5/5 (12)
- Getting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsFrom EverandGetting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsRating: 3.5 out of 5 stars3.5/5 (8)
- Development of Questionnaires for Quantitative Medical ResearchFrom EverandDevelopment of Questionnaires for Quantitative Medical ResearchNo ratings yet
- Microbiological Quality of FoodsFrom EverandMicrobiological Quality of FoodsL SlanetzNo ratings yet
- The Varicose Veins Mastery Bible: Your Blueprint for Complete Varicose Veins ManagementFrom EverandThe Varicose Veins Mastery Bible: Your Blueprint for Complete Varicose Veins ManagementNo ratings yet