You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- SAP EAM-PM - Fleet Management - Main ProcessDocument2 pagesSAP EAM-PM - Fleet Management - Main Processleoaug67% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 6 QualitiesDocument5 pages6 Qualitiesrahmaa04No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Aws Final ReportDocument27 pagesAws Final Reportkiswah computers100% (2)
- Basic Concepts of Applied Motor Learning and Performance: GROUP 2 - Presenter Name: CALICDAN, PIADocument44 pagesBasic Concepts of Applied Motor Learning and Performance: GROUP 2 - Presenter Name: CALICDAN, PIAPia Mae Zenith Calicdan100% (1)
- Week8 Bau Coop DM DigitalproductDocument23 pagesWeek8 Bau Coop DM DigitalproductOnur MutluayNo ratings yet
- BGP Neighbor Adjacency StatesDocument3 pagesBGP Neighbor Adjacency StatesSon Tran Hong NamNo ratings yet
- PE: Larong-LahiDocument10 pagesPE: Larong-LahiKRISTEL CAZANDRA EMPASNo ratings yet
- Essential IeltsDocument112 pagesEssential IeltsHtike HtikeNo ratings yet
- Car ParkingDocument30 pagesCar ParkingDHINESH ITNo ratings yet
- DIETARY PRINCIPLES FOR LIFE Presentation & Research File MSU 2018Document30 pagesDIETARY PRINCIPLES FOR LIFE Presentation & Research File MSU 2018Siphiwe SitholeNo ratings yet
- Neoflo 1-68i (IO)Document3 pagesNeoflo 1-68i (IO)Kinni ShenoldNo ratings yet
- Catalogo Telefonia Movil 2008Document220 pagesCatalogo Telefonia Movil 2008pmn_23No ratings yet
- Adsorption ChillerDocument19 pagesAdsorption Chilleragalvan1311No ratings yet
- Viper 20000 PCDocument176 pagesViper 20000 PCrop703406No ratings yet
- Sons and Lovers Chapter 2 SummaryDocument2 pagesSons and Lovers Chapter 2 SummaryLuiseNo ratings yet
- Newsletter 20 24th February 2023Document14 pagesNewsletter 20 24th February 2023Ishtiaq LodhiNo ratings yet
- Nbde Part 1 NerveDocument12 pagesNbde Part 1 NerveMrunal DoiphodeNo ratings yet
- Neonatal JaundiceDocument56 pagesNeonatal Jaundicesuardiman acoNo ratings yet
- Product Manual For Line Operated Three Phase A.C. Motors (Ie Code) "Efficiency Classes and Performance Specification" ACCORDING TO IS 12615:2018Document8 pagesProduct Manual For Line Operated Three Phase A.C. Motors (Ie Code) "Efficiency Classes and Performance Specification" ACCORDING TO IS 12615:2018Arun ArumugamNo ratings yet
- Phacodynamics: Phacoemulsification For Residents Unpad - Cicendo Eye Hospital 2020Document40 pagesPhacodynamics: Phacoemulsification For Residents Unpad - Cicendo Eye Hospital 2020GabrielaNo ratings yet
- Medtronic Company OverviewDocument35 pagesMedtronic Company OverviewIhsan DisiniNo ratings yet
- Proforma GC6033 Sem 2 2019202020 13 Mac 2020-20200317093134 PDFDocument4 pagesProforma GC6033 Sem 2 2019202020 13 Mac 2020-20200317093134 PDFTanicshaNo ratings yet
- Analysis and Design of A Three Phase Sliding Mode Controller For A Shunt Active Power FilterDocument5 pagesAnalysis and Design of A Three Phase Sliding Mode Controller For A Shunt Active Power Filterphoenix226No ratings yet
- Smoham CVDocument8 pagesSmoham CVOmid Kazemzadeh KhoeeNo ratings yet
- 17 4PH PDFDocument12 pages17 4PH PDFa.n.87711990No ratings yet
- Military Tactics + Gun PowderDocument6 pagesMilitary Tactics + Gun Powdermaham sanayaNo ratings yet
- Dislike of Math Thesis (FINAL VERSION)Document35 pagesDislike of Math Thesis (FINAL VERSION)api-382012694% (36)
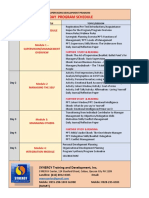
- 5 Days 1page Sched of SDPDocument2 pages5 Days 1page Sched of SDPJam MacacuaNo ratings yet
- Life As Cinema by Dzongsar Jamyang Khyentse RinpocheDocument2 pagesLife As Cinema by Dzongsar Jamyang Khyentse RinpochemiodakiniNo ratings yet
- Eng Moti 0Document2 pagesEng Moti 0Barış ErçeNo ratings yet