You might also like
- A Delivery Room Write-UpDocument24 pagesA Delivery Room Write-UpDyanne BautistaNo ratings yet
- High Risk Pregnancy Review QuestionsDocument59 pagesHigh Risk Pregnancy Review Questionsmitted100% (1)
- Theories Related To Maternal and Child NursingDocument24 pagesTheories Related To Maternal and Child NursingAubrey Dynise C. Torralba100% (1)
- 1 - Chapter 1-Introduction To Maternal and Child Health NursingqweqeDocument34 pages1 - Chapter 1-Introduction To Maternal and Child Health NursingqweqeSherwin Mike Quijote100% (4)
- Essential Intrapartum and Newborn CareDocument27 pagesEssential Intrapartum and Newborn Careteabagman100% (2)
- Lesson Plan On Uterine Abnormality and Displacement: B.SC Nursing StudentsDocument20 pagesLesson Plan On Uterine Abnormality and Displacement: B.SC Nursing StudentsKinjal VasavaNo ratings yet
- Theories of Labor Ons-EtDocument19 pagesTheories of Labor Ons-EtHeron BayaninNo ratings yet
- Drug Study On Labor and DeliveryDocument4 pagesDrug Study On Labor and DeliveryJune Dumdumaya67% (3)
- Problems With The PassengerDocument65 pagesProblems With The Passengermark Orpilla100% (1)
- Fetal Skull - Madam JustinaDocument11 pagesFetal Skull - Madam JustinaNana Yunus67% (3)
- Nursing Care Plan Abruptio PlacentaeDocument2 pagesNursing Care Plan Abruptio PlacentaeWann WannNo ratings yet
- Subinvolution: Unit: IXDocument12 pagesSubinvolution: Unit: IXmikegrace0250% (2)
- Care - of - Mother - Child - and - Adolescent 2Document48 pagesCare - of - Mother - Child - and - Adolescent 2Jmarie Brillantes PopiocoNo ratings yet
- Partograph: Jillian A. Bejoc, MSN, RNDocument44 pagesPartograph: Jillian A. Bejoc, MSN, RNJiezl Abellano AfinidadNo ratings yet
- Fetal SkullDocument17 pagesFetal SkullCham_Aley100% (1)
- Management of First Stage of LaborDocument19 pagesManagement of First Stage of Laborjencymol100% (8)
- Premonitory Stage of LabourDocument23 pagesPremonitory Stage of LabourAnnapurna Dangeti100% (1)
- Problems With The PassagewayDocument43 pagesProblems With The PassagewayMathew Beniga Gaco92% (12)
- Theories of Onset of LabourDocument36 pagesTheories of Onset of LabourmitnexusNo ratings yet
- Gestational AgeDocument6 pagesGestational AgemhuniswellNo ratings yet
- Mechanism of Normal LabourDocument2 pagesMechanism of Normal Labourswethashaki100% (2)
- Nursing Care of The Client With High-Risk Labor & DeliveryDocument10 pagesNursing Care of The Client With High-Risk Labor & DeliveryWilbert CabanbanNo ratings yet
- NCM 109N: Frameworks For Maternal & Child Health NursingDocument37 pagesNCM 109N: Frameworks For Maternal & Child Health NursingZudota100% (1)
- Rubin's TheoryDocument3 pagesRubin's TheoryBeerna Grande50% (2)
- Notes On Obstetrics: Normal Labor (Theories of Labor Onset)Document22 pagesNotes On Obstetrics: Normal Labor (Theories of Labor Onset)Jobelle Acena100% (1)
- Face PresentationDocument6 pagesFace PresentationNishaThakuriNo ratings yet
- Unang YakapDocument3 pagesUnang YakapBernadeth Labrador100% (1)
- Intrapartal - Theories of LaborDocument21 pagesIntrapartal - Theories of LaborJan Oliver YaresNo ratings yet
- Purpose:: Procedure: Rationale: Introduce Yourself and Inform Pregnant Woman About The ProcedureDocument5 pagesPurpose:: Procedure: Rationale: Introduce Yourself and Inform Pregnant Woman About The ProcedureArmySapphire100% (1)
- Signs of Placental SeparationDocument1 pageSigns of Placental SeparationMalou Yap Buot0% (1)
- Premature LabourDocument29 pagesPremature LabourSanthosh.S.U100% (1)
- Normal Labor Unit 2.1Document19 pagesNormal Labor Unit 2.1NishaThakuri100% (1)
- 10.theories of LaborDocument18 pages10.theories of LaborJulia Ramos100% (1)
- I. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsDocument5 pagesI. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsSophia Loraine Dorone Jesura100% (1)
- Reva Rubin Maternal Role Attainment TheoryDocument4 pagesReva Rubin Maternal Role Attainment TheoryLeonard LigutomNo ratings yet
- Nursing Care of The Family Having Difficulty Conceiving A ChildDocument10 pagesNursing Care of The Family Having Difficulty Conceiving A ChildAndrei Borata100% (2)
- Health Teaching During PergnancyDocument4 pagesHealth Teaching During PergnancyAnuradha MauryaNo ratings yet
- Prelim NCM 109 Lecture HandoutsDocument21 pagesPrelim NCM 109 Lecture HandoutsLillabin71% (7)
- NCP Post PartumDocument11 pagesNCP Post PartumClaire Dayrit100% (1)
- Final Nursing Care PlanDocument8 pagesFinal Nursing Care PlanDickson,Emilia Jade100% (1)
- Family Planning MethodDocument105 pagesFamily Planning MethodKailash NagarNo ratings yet
- Difference BTW Nursing & Educational ProcessDocument3 pagesDifference BTW Nursing & Educational ProcessShubhi VaivhareNo ratings yet
- Framework For Maternal and Child Health NursingDocument10 pagesFramework For Maternal and Child Health NursingSHERYL TEMPLANo ratings yet
- Maternal and Child Health Nursing Is Family-Centered Assessment DataDocument5 pagesMaternal and Child Health Nursing Is Family-Centered Assessment DataWendell Gian GolezNo ratings yet
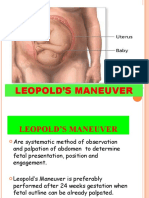
- Leopold's ManeuverDocument22 pagesLeopold's ManeuverArlene Cerdeña Salceda100% (1)
- Theories of Labor OnsetDocument4 pagesTheories of Labor OnsetCzarina PorciunculaNo ratings yet
- PartographDocument6 pagesPartographalyssa marie salcedo100% (1)
- Case Study On Observation and Newborn CareDocument38 pagesCase Study On Observation and Newborn CarePiyush Dutta100% (2)
- Immediate Care of The NewbornDocument4 pagesImmediate Care of The NewbornMichelle GambolNo ratings yet
- Nursing Care of The Postpartum ClientDocument13 pagesNursing Care of The Postpartum ClientLyca Mae AurelioNo ratings yet
- Role and Function of The MidwifeDocument30 pagesRole and Function of The MidwifeRose Ann86% (14)
- Anatomy and Physiology of Breech PresentationDocument2 pagesAnatomy and Physiology of Breech Presentationeskempertus0% (2)
- Leopolds and FetalDocument7 pagesLeopolds and Fetaltyche100% (1)
- Anatomy and Physiology of PlacentaDocument5 pagesAnatomy and Physiology of PlacentaAdrianne Basa100% (1)
- Pathophysiology of NSVDDocument2 pagesPathophysiology of NSVDLenjun83% (6)
- Labor and DeliveryDocument6 pagesLabor and DeliveryKenny NadelaNo ratings yet
- n3633 MM Module 1 Unit 1Document71 pagesn3633 MM Module 1 Unit 1jonscastro450No ratings yet
- Labor and Delivery (Final)Document209 pagesLabor and Delivery (Final)Angel Gabriel FornillosNo ratings yet
- Theories and 6 Ps of LaborDocument80 pagesTheories and 6 Ps of LaborEpilepsy ManNo ratings yet
- CH 15 Labor and Birth Part 1 HANDOUTDocument5 pagesCH 15 Labor and Birth Part 1 HANDOUTEula ReyesNo ratings yet
- Chapter 25 NotesDocument7 pagesChapter 25 NotesJori Domini Llacuna AwayanNo ratings yet
- Female Reproductive HealthDocument276 pagesFemale Reproductive HealthviannikkkyNo ratings yet
- N227F - 2004 - OBS Lecture 1 - Introduction To Obstetric Nursing Lecture NotesDocument17 pagesN227F - 2004 - OBS Lecture 1 - Introduction To Obstetric Nursing Lecture NotesPriscilla NgNo ratings yet
- Ca Cervix: DR Monika Teresa Prasetyo DR Sienny Amelia KwokDocument73 pagesCa Cervix: DR Monika Teresa Prasetyo DR Sienny Amelia KwokZien SienNo ratings yet
- Lower Genital Tract InfectionDocument3 pagesLower Genital Tract InfectiondanielNo ratings yet
- 10a Aepcc Guidelines ColposDocument80 pages10a Aepcc Guidelines ColposReginaNo ratings yet
- Genital Prolapse: Unit - V 2K15Document58 pagesGenital Prolapse: Unit - V 2K15sushma nakkinaNo ratings yet
- IDPS Chapter 15Document10 pagesIDPS Chapter 15002No ratings yet
- Vital SignsDocument5 pagesVital SignsTUKH-LDRNo ratings yet
- Maternal Lec Semi-FinalsDocument433 pagesMaternal Lec Semi-FinalsTrishaNo ratings yet
- Maternal Health/ OB Final Exam Study GuideDocument252 pagesMaternal Health/ OB Final Exam Study Guidelorrainenxumalo0% (2)
- II. PATHOPHYSIOLOGY (Schematic Diagram) : Risk Factors Predisposing FactorsDocument3 pagesII. PATHOPHYSIOLOGY (Schematic Diagram) : Risk Factors Predisposing FactorsYongNo ratings yet
- Abnormal Uterine ActionDocument96 pagesAbnormal Uterine ActionN. Siva100% (2)
- Pap SmearDocument8 pagesPap Smearsmv2No ratings yet
- Pelvic ExaminationDocument3 pagesPelvic ExaminationAdisorn ChaikitNo ratings yet
- Definition of Placenta PreviaDocument3 pagesDefinition of Placenta Previashan6ersNo ratings yet
- Birth Canal Injuries Final LectureDocument28 pagesBirth Canal Injuries Final LectureAnjali Rahul AjmeriNo ratings yet
- Acute Uterine InversionDocument6 pagesAcute Uterine InversionBima GhovaroliyNo ratings yet
- Stuffed NurseDocument42 pagesStuffed NurseG-s HO CKNo ratings yet
- Surgicopath June, 2018 FinalDocument115 pagesSurgicopath June, 2018 FinalPencenk AzznewNo ratings yet
- Obstetric Safety ProtocolsDocument10 pagesObstetric Safety ProtocolsApril LilianNo ratings yet
- Family Planning Methods - LatestDocument59 pagesFamily Planning Methods - LatestGenevieve VillaflorNo ratings yet
- Chapter 16: Labor and BirthDocument27 pagesChapter 16: Labor and Birthejyoung928No ratings yet
- Labor Part 1Document7 pagesLabor Part 1RANDY ERNEST GESTOSANINo ratings yet
- Anatomy Changes During PregnancyDocument36 pagesAnatomy Changes During PregnancyFirdaus Septiawan100% (1)
- Obg Qus Set 3Document24 pagesObg Qus Set 3RajaNo ratings yet
- Cervical Screening: Guidance For The Training of Cervical Sample TakersDocument14 pagesCervical Screening: Guidance For The Training of Cervical Sample TakersCalinnescuNo ratings yet
- Induction of Labor PDFDocument8 pagesInduction of Labor PDFGustomo PanantroNo ratings yet
- Instruments Obs & Gynea PDFDocument19 pagesInstruments Obs & Gynea PDFVibes Usmlee100% (1)
- Ob Supplement Handout by DR - Chris SorianoDocument33 pagesOb Supplement Handout by DR - Chris SorianoHedley Chua75% (4)