You might also like
- Atropine Sulfate for Bradycardia and PoisoningDocument4 pagesAtropine Sulfate for Bradycardia and PoisoningSuraya_Mohamed_3281No ratings yet
- Drug StudyDocument7 pagesDrug StudydivineNo ratings yet
- Drug Study - Atropine Sulfate (Atropair)Document2 pagesDrug Study - Atropine Sulfate (Atropair)mikErlh100% (1)
- AtropairDocument2 pagesAtropairianecunarNo ratings yet
- Side Effects:: AtropineDocument7 pagesSide Effects:: AtropinekletadaNo ratings yet
- Preparation of Drug Profile of AtropineDocument8 pagesPreparation of Drug Profile of AtropineSufian AhmadNo ratings yet
- Drug Book On EmergencyDocument21 pagesDrug Book On EmergencyDimpal Choudhary100% (4)
- Cholinergic Antagonists GuideDocument49 pagesCholinergic Antagonists GuideGde Ananda ArmanditaNo ratings yet
- Drug StudyDocument43 pagesDrug StudyMamot MotNo ratings yet
- Epinephrine: Uses, Dosages, Side EffectsDocument15 pagesEpinephrine: Uses, Dosages, Side EffectsDennise Juayang100% (1)
- Drug StudyDocument43 pagesDrug Studyapi-3818438100% (2)
- Drugs Fall 2014: Pharm ListDocument31 pagesDrugs Fall 2014: Pharm Listashleynorris1403No ratings yet
- 3 ParasympatholyticsDocument35 pages3 ParasympatholyticsSudhakar LakavathNo ratings yet
- Dept - Farmakologi & Terapeutik Fak - Kedokteran U S U Medan: Prof - Dr.H.Aznan Lelo PHD - SPFK DR - Datten Bangun MSC, SPFKDocument62 pagesDept - Farmakologi & Terapeutik Fak - Kedokteran U S U Medan: Prof - Dr.H.Aznan Lelo PHD - SPFK DR - Datten Bangun MSC, SPFKAnonymous zZrGTONhNo ratings yet
- 2 19 REMSA Paramedic Program Drug ListDocument49 pages2 19 REMSA Paramedic Program Drug ListEmily KeenNo ratings yet
- Anticholinergic DrugsDocument12 pagesAnticholinergic DrugsMARCOS ALEJANDRO CHAMORRO TRUJILLONo ratings yet
- Drug Study On Emergency DrugsDocument16 pagesDrug Study On Emergency DrugsJosepNo ratings yet
- Emergency DrugsDocument15 pagesEmergency Drugsjheverly123100% (1)
- Drug Study On Emergency DrugsDocument15 pagesDrug Study On Emergency DrugsJAy TootNo ratings yet
- Pharmacology List 2018Document30 pagesPharmacology List 2018C ScribNo ratings yet
- Glyphosate Poisoning: Presenter: Prabu Medical Officer: Dr. NG KL Specialist: DR KauthmanDocument39 pagesGlyphosate Poisoning: Presenter: Prabu Medical Officer: Dr. NG KL Specialist: DR KauthmanPrabu PonuduraiNo ratings yet
- Emergency Drugs Drug StudyDocument15 pagesEmergency Drugs Drug StudyCathrine Sandile Tangwara100% (1)
- Adult: IV: Bradycardia PoisoningDocument28 pagesAdult: IV: Bradycardia PoisoningArthur William Tell BarbaNo ratings yet
- Emergency Drugs: Oleh: Tiffany Chang Kepaniteraan Klinik Departemen Anestesi Dan Reanimasi Rspad Gatot SoebrotoDocument22 pagesEmergency Drugs: Oleh: Tiffany Chang Kepaniteraan Klinik Departemen Anestesi Dan Reanimasi Rspad Gatot Soebrototiffanychang0510No ratings yet
- AtropineDocument1 pageAtropinejkim28No ratings yet
- AtropineDocument4 pagesAtropineAnung RespatiNo ratings yet
- Anticholinergic PsychotomimeticsDocument126 pagesAnticholinergic PsychotomimeticsLuděk Spurný100% (1)
- Week 13 Drug CardsDocument5 pagesWeek 13 Drug CardsPRECIOUS wardNo ratings yet
- Action: Indications:: Drug: Oxygen Class of Medication: Oxidizing Agent (Gas)Document6 pagesAction: Indications:: Drug: Oxygen Class of Medication: Oxidizing Agent (Gas)Andreas100% (2)
- BLS Pharmacology PowerpointDocument18 pagesBLS Pharmacology Powerpointmerabtialaeddine5No ratings yet
- Drugs VivaDocument7 pagesDrugs VivaachyutsharmaNo ratings yet
- Availability: Psychopharmacology Chlorpromazine HydrochlorideDocument10 pagesAvailability: Psychopharmacology Chlorpromazine HydrochlorideWendz Palma-TudaNo ratings yet
- Atropine Drug ProfileDocument2 pagesAtropine Drug ProfileShahpmdNo ratings yet
- PimozideDocument5 pagesPimozideMega AnandaNo ratings yet
- Cholinergic AntagonistsDocument18 pagesCholinergic AntagonistsApurba Sarker Apu100% (1)
- AEA - Ambulance Emergency Assistant - ProtocolsDocument12 pagesAEA - Ambulance Emergency Assistant - ProtocolsM Gavin100% (4)
- Drug Study On EPINEPHRINEDocument6 pagesDrug Study On EPINEPHRINEshadow gonzalezNo ratings yet
- TOP DRUGS - Doc Version 1Document12 pagesTOP DRUGS - Doc Version 1Charme Jean RaygonNo ratings yet
- Top DrugsDocument12 pagesTop DrugsStephanie Villanueva AdvinculaNo ratings yet
- Pharma CAL Lab Dog BP Expt.Document14 pagesPharma CAL Lab Dog BP Expt.sibananda palNo ratings yet
- Drug StudyDocument9 pagesDrug StudyChristine PunsalanNo ratings yet
- EpinephrineDocument6 pagesEpinephrineapi-3797941100% (2)
- Drug Study FORTDocument3 pagesDrug Study FORTLysa Mae EleazarNo ratings yet
- BricanylDocument4 pagesBricanylianecunarNo ratings yet
- Dept - Farmakologi & Terapeutik Fak - Kedokteran U H N Medan: DR - Datten Bangun MSC, SPFKDocument57 pagesDept - Farmakologi & Terapeutik Fak - Kedokteran U H N Medan: DR - Datten Bangun MSC, SPFKBRI KUNo ratings yet
- Atropine SulfateDocument6 pagesAtropine SulfateManelle SingzonNo ratings yet
- Parasympatholytics: Atropine and its UsesDocument13 pagesParasympatholytics: Atropine and its UsesareebwaheedNo ratings yet
- Atropine Sulfate InjectionDocument4 pagesAtropine Sulfate InjectionIrawanMarlyNo ratings yet
- Obat-Obat Emergency: DR T. Mamfaluti, SPPDDocument36 pagesObat-Obat Emergency: DR T. Mamfaluti, SPPDIqbal AminNo ratings yet
- Anticholinergic: Anticholinergics: Generic and Brand NamesDocument6 pagesAnticholinergic: Anticholinergics: Generic and Brand NamesSaffery Gly LayuganNo ratings yet
- Drug File SupriyaDocument36 pagesDrug File SupriyaSalim MinjNo ratings yet
- 2 Antimuscarinic Drugs Dr. Dubey 2011Document17 pages2 Antimuscarinic Drugs Dr. Dubey 2011ecc bafNo ratings yet
- Breast Cancer: Melatonin Helps to: Prevent Cancer, Avoid Drug Resistance, Stop MetastasisFrom EverandBreast Cancer: Melatonin Helps to: Prevent Cancer, Avoid Drug Resistance, Stop MetastasisNo ratings yet
- Pembelian Alat Dan Bahan Di Promedika SamarindaDocument5 pagesPembelian Alat Dan Bahan Di Promedika SamarindaAndrean LinataNo ratings yet
- No Nama Alat Jumlah Sumber Alat Harga AlatDocument1 pageNo Nama Alat Jumlah Sumber Alat Harga AlatAndrean LinataNo ratings yet
- Consolidated General Application Form Immigration Regulation DivisionDocument1 pageConsolidated General Application Form Immigration Regulation DivisionAndrean LinataNo ratings yet
- PesanestetikaDocument2 pagesPesanestetikaAndrean LinataNo ratings yet
- No Nama Alat Jumlah Sumber Alat Harga AlatDocument1 pageNo Nama Alat Jumlah Sumber Alat Harga AlatAndrean LinataNo ratings yet
- Mary Grace Anne A. CalvaridoDocument15 pagesMary Grace Anne A. CalvaridoAndrean LinataNo ratings yet
- Efficacy of Bleomycin for Periungual Warts after CO2 LaserDocument23 pagesEfficacy of Bleomycin for Periungual Warts after CO2 LaserAndrean LinataNo ratings yet
- Reporting in Phototherapy-CompiledDocument78 pagesReporting in Phototherapy-CompiledAndrean LinataNo ratings yet
- Department of Dermatology Ospital NG Maynila Medical Center Pamantasan NG Lungsod NG MaynilaDocument21 pagesDepartment of Dermatology Ospital NG Maynila Medical Center Pamantasan NG Lungsod NG MaynilaAndrean LinataNo ratings yet
- 10 1111@dth 13034Document6 pages10 1111@dth 13034Andrean LinataNo ratings yet
- FINAL Research Androgenetic AlopeciaDocument42 pagesFINAL Research Androgenetic AlopeciaAndrean LinataNo ratings yet
- Research 31233Document5 pagesResearch 31233Andrean LinataNo ratings yet
- Common Nevus: Clinical Diagnosis: Andrean Linata Ospital NG Maynila Medical CenterDocument26 pagesCommon Nevus: Clinical Diagnosis: Andrean Linata Ospital NG Maynila Medical CenterAndrean LinataNo ratings yet
- Photodiagnosis and Photodynamic Therapy: SciencedirectDocument5 pagesPhotodiagnosis and Photodynamic Therapy: SciencedirectAndrean LinataNo ratings yet
- Giacaman2019 Article UseOfTopicalNitricZincComplexSDocument6 pagesGiacaman2019 Article UseOfTopicalNitricZincComplexSAndrean LinataNo ratings yet
- Therapeutic Evaluation of Efficacy of Intralesional Bleomycin in Common Warts Including Palmo-Plantar and Periungual Warts: A Prospective StudyDocument9 pagesTherapeutic Evaluation of Efficacy of Intralesional Bleomycin in Common Warts Including Palmo-Plantar and Periungual Warts: A Prospective StudyAndrean LinataNo ratings yet
- Oamjms 7 214Document3 pagesOamjms 7 214Andrean LinataNo ratings yet
- PistolsHandbook12 10 15Document157 pagesPistolsHandbook12 10 15SanelaBožičkovićNo ratings yet
- Case Report Tyroid CA SkinDocument6 pagesCase Report Tyroid CA SkinAndrean LinataNo ratings yet
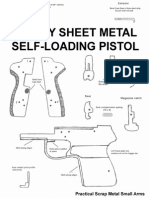
- The DIY Sheet Metal Self-Loading Pistol (Practical Scrap Metal Small Arms) PDFDocument15 pagesThe DIY Sheet Metal Self-Loading Pistol (Practical Scrap Metal Small Arms) PDFgunpdfs93% (121)
- Case Report Tyroid CA SkinDocument6 pagesCase Report Tyroid CA SkinAndrean LinataNo ratings yet
- Latihan Soal 2Document2 pagesLatihan Soal 2Andrean LinataNo ratings yet
- Nail Growth and DifferentiationDocument5 pagesNail Growth and DifferentiationAndrean LinataNo ratings yet
- Nelson Essentials - EncephalitisDocument8 pagesNelson Essentials - EncephalitisAndrean LinataNo ratings yet
- Eritrasma BelajarDocument6 pagesEritrasma BelajarAndrean LinataNo ratings yet
- Total: TotalDocument1 pageTotal: TotalAndrean LinataNo ratings yet
- Nelson Essentials - TuberculosisDocument14 pagesNelson Essentials - TuberculosisAndrean LinataNo ratings yet
- Jurding THTDocument18 pagesJurding THTAndrean LinataNo ratings yet
- Oh My GoodiesDocument1 pageOh My GoodiesAndrean LinataNo ratings yet
- Guidelines TBC TerbaruDocument160 pagesGuidelines TBC TerbaruSutoto MoeljadiNo ratings yet