You might also like
- Parenteral Nutrition Manual June 2018 WebsiteDocument85 pagesParenteral Nutrition Manual June 2018 WebsitemildaNo ratings yet
- Minor AilmentsDocument16 pagesMinor AilmentsSujatha J Jayabal86% (7)
- Care Plan On PneumoniaDocument22 pagesCare Plan On PneumoniaDimpal Choudhary100% (3)
- Care Plan ON Periampullary Carcinoma: SUBMITTED TO-Ms. Tarika Sharma SUBMITTED BY-Mr. DeepakDocument27 pagesCare Plan ON Periampullary Carcinoma: SUBMITTED TO-Ms. Tarika Sharma SUBMITTED BY-Mr. Deepakamit100% (3)
- Careplan Medication ListDocument17 pagesCareplan Medication ListGiorgia ScorsoneNo ratings yet
- Case Presentation On TOFDocument19 pagesCase Presentation On TOFJay PaulNo ratings yet
- Procedure On Chest PhysiotherapyDocument13 pagesProcedure On Chest PhysiotherapyDimpal ChoudharyNo ratings yet
- Emergency Drugs Drug StudyDocument15 pagesEmergency Drugs Drug StudyCathrine Sandile Tangwara100% (1)
- Drug StudyDocument10 pagesDrug StudyBandana RajpootNo ratings yet
- Drug Study ON Cabergolin EDocument4 pagesDrug Study ON Cabergolin ESimran SimzNo ratings yet
- AtropineDocument13 pagesAtropineMostafa HassanNo ratings yet
- Structured Teaching Programme On Prevention of Ventilator Associated PneumoniaDocument15 pagesStructured Teaching Programme On Prevention of Ventilator Associated PneumoniaSagiraju Srinu100% (1)
- Drug Study TBDocument5 pagesDrug Study TBSanvar Mal SoniNo ratings yet
- Nebulization and Steam InhalationDocument31 pagesNebulization and Steam InhalationManisha Thakur100% (1)
- Drugs in Pediatrics: Submitted By: Prerna Sharma M.SC Nursing, 4 SemesterDocument42 pagesDrugs in Pediatrics: Submitted By: Prerna Sharma M.SC Nursing, 4 SemesterPrernaSharma100% (1)
- DrugsDocument5 pagesDrugsdeepika kushwah100% (1)
- Name of Drug Dose Action Indication Contraindicatio N Side Effect Nurses ResponsibilityDocument22 pagesName of Drug Dose Action Indication Contraindicatio N Side Effect Nurses ResponsibilityPunam PalNo ratings yet
- Nursing Management: OF ArteriosclerosisDocument6 pagesNursing Management: OF ArteriosclerosisANCHAL SHARMANo ratings yet
- AdrenalineDocument13 pagesAdrenalineMobahil AhmadNo ratings yet
- Case Management of Ari at PHC LevelDocument29 pagesCase Management of Ari at PHC Levelapi-3823785No ratings yet
- Drug Presentation AtropineDocument6 pagesDrug Presentation AtropineShivam Malik100% (1)
- Care of Child With Head InjuryDocument34 pagesCare of Child With Head InjurySHAFIQNo ratings yet
- ReportDocument20 pagesReportAshwini Patil0% (1)
- Drug Presentation On: Aminoven: Submitted To Submitted byDocument6 pagesDrug Presentation On: Aminoven: Submitted To Submitted byShilpi SinghNo ratings yet
- MSN II 01.7.2020-OSCE in Instillation of Ear DropsDocument3 pagesMSN II 01.7.2020-OSCE in Instillation of Ear DropsYAMINIPRIYANNo ratings yet
- Bowel Wash: Child Health Nursing ProcedureDocument4 pagesBowel Wash: Child Health Nursing ProcedureEllen Angel100% (1)
- Final ColistinDocument3 pagesFinal ColistinGwyn RosalesNo ratings yet
- 13th & 14th WK - Oxygen Therapy With VideoDocument89 pages13th & 14th WK - Oxygen Therapy With VideoJesus Mario Lopez100% (1)
- Identification Data of PatientDocument8 pagesIdentification Data of Patientanimesh panda50% (2)
- CVADocument22 pagesCVAPankaj Shahi100% (1)
- Cardiovascular Assessment: Assessment Uses of CVS AssessmentDocument8 pagesCardiovascular Assessment: Assessment Uses of CVS AssessmentKawaljit KaurNo ratings yet
- Eye Banking OphthalmologyDocument21 pagesEye Banking Ophthalmologyvivekrajbhilai5850100% (2)
- Crash Cart Drugs 1Document23 pagesCrash Cart Drugs 1Kristiina MakinenNo ratings yet
- BloodDocument49 pagesBloodvruttika parmar100% (3)
- Cardaic Emergency Drugs.Document13 pagesCardaic Emergency Drugs.Alma SusanNo ratings yet
- StreptokinaseDocument18 pagesStreptokinasedickyNo ratings yet
- SuctionDocument15 pagesSuctionMissy Shona100% (1)
- Management of Dengue FeverDocument16 pagesManagement of Dengue FeverSupriyati Rahayu0% (1)
- Skill 11 (1) ..Collection of Stool SpecimenDocument1 pageSkill 11 (1) ..Collection of Stool SpecimennetsquadNo ratings yet
- Care of Unconscious PatientDocument5 pagesCare of Unconscious PatientRuchika Kaushal67% (3)
- AdrenalineDocument14 pagesAdrenalineOmar AyoubNo ratings yet
- Share ANTIDOTE M1 TCON UNION'21Document118 pagesShare ANTIDOTE M1 TCON UNION'21Sandra Ann Biju100% (1)
- Lesson Plan MSN 1Document14 pagesLesson Plan MSN 1SHREE SWAMINARAYAN NURSING COLLEGE CHIKHLINo ratings yet
- Case Presentation On Myocardial InfarctionDocument27 pagesCase Presentation On Myocardial InfarctionAmit RanjanNo ratings yet
- Care of Child With IncubatorDocument26 pagesCare of Child With IncubatorSabita Paudel100% (2)
- Case Study FormatDocument15 pagesCase Study FormatLavie GangwarNo ratings yet
- History of MSNDocument20 pagesHistory of MSNSyamVRNo ratings yet
- Types of Reconstructive & Cosmetic SurgeryDocument28 pagesTypes of Reconstructive & Cosmetic SurgerySimon JosanNo ratings yet
- Endotracheal Tube InsertionDocument41 pagesEndotracheal Tube Insertionrufusprasanth_rachaprolu88% (16)
- Status Asthmaticus DefinitionDocument2 pagesStatus Asthmaticus Definitionhemaanandhy0% (1)
- Defibrillation and Electrical CardioversionDocument27 pagesDefibrillation and Electrical CardioversionYui Hirasawa100% (1)
- Abdominal ParacentesisDocument4 pagesAbdominal ParacentesisRashmi C S100% (1)
- Pyodermas 2014Document41 pagesPyodermas 2014Dudy Humaedi100% (6)
- Observation Report On ENTDocument15 pagesObservation Report On ENTEsther Kipgen100% (2)
- Antidiuretic DrugsDocument4 pagesAntidiuretic DrugsNavjot BrarNo ratings yet
- CPR PPT FinalDocument83 pagesCPR PPT FinalSimran Josan100% (2)
- Crash CartDocument12 pagesCrash CartMarcus Philip Gonzales100% (1)
- Cardiac System AssessmentDocument14 pagesCardiac System AssessmentValarmathi100% (1)
- Foot and Hand Care: Learning ObjectivesDocument7 pagesFoot and Hand Care: Learning ObjectivesNITHYAPREMINI100% (1)
- Westfort College of Nursing Osce-Cardiopulmonary ResuscitationDocument1 pageWestfort College of Nursing Osce-Cardiopulmonary Resuscitationvishnu100% (1)
- Drug StudyDocument4 pagesDrug StudyJeboy SadioaNo ratings yet
- Side Effects:: AtropineDocument7 pagesSide Effects:: AtropinekletadaNo ratings yet
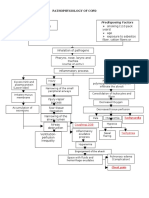
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyNo ratings yet
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Document70 pagesPeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyNo ratings yet
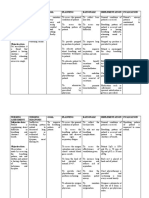
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- Pulmonary FibrosisDocument4 pagesPulmonary FibrosisDimpal Choudhary100% (2)
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument4 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal ChoudharyNo ratings yet
- Pathophysiology of PneumoniaDocument4 pagesPathophysiology of PneumoniaDimpal ChoudharyNo ratings yet
- Pathophysiology of Pleural EffusionDocument1 pagePathophysiology of Pleural EffusionDimpal ChoudharyNo ratings yet
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyNo ratings yet
- Lumber Puncture ProcedureDocument8 pagesLumber Puncture ProcedureDimpal ChoudharyNo ratings yet
- Congenital Heart DiseaseDocument82 pagesCongenital Heart DiseaseDimpal ChoudharyNo ratings yet
- Nursing EducationDocument19 pagesNursing EducationDimpal ChoudharyNo ratings yet
- Uninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Document6 pagesUninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Dimpal ChoudharyNo ratings yet
- Preparation OF Group Work: Netaji Subhash College of NursingDocument7 pagesPreparation OF Group Work: Netaji Subhash College of NursingDimpal ChoudharyNo ratings yet
- Bladder IrrigationDocument5 pagesBladder IrrigationDimpal ChoudharyNo ratings yet
- Self-Directed LearningDocument18 pagesSelf-Directed LearningDimpal ChoudharyNo ratings yet
- Introduction-:: Time Specific Objective Content Av AidsDocument7 pagesIntroduction-:: Time Specific Objective Content Av AidsDimpal ChoudharyNo ratings yet
- Polycythemia Vera: What Are The Symptoms of Polycythemia?Document10 pagesPolycythemia Vera: What Are The Symptoms of Polycythemia?Dimpal ChoudharyNo ratings yet
- It Is of Two Types Natural Disaster Man - Made DisasterDocument4 pagesIt Is of Two Types Natural Disaster Man - Made DisasterDimpal ChoudharyNo ratings yet
- Differential Diagnosis For The Dermatologist PDFDocument1,352 pagesDifferential Diagnosis For The Dermatologist PDFAndri Sati Siregar80% (5)
- Aaos PDFDocument4 pagesAaos PDFWisnu CahyoNo ratings yet
- Nursing Care Plan For Hip Fracture Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationDocument1 pageNursing Care Plan For Hip Fracture Assessment Diagnosis Rationale Goal & Objectives Interventions Rationale EvaluationJaylord Verazon100% (1)
- Cephalopelvic DisproportionDocument6 pagesCephalopelvic DisproportionQuennie Alam100% (1)
- SMOFlipid 20%Document4 pagesSMOFlipid 20%Meta Hanindita NugrohoNo ratings yet
- WP Contentuploads202208ExportFinalProgram 19082022113125 PDFDocument423 pagesWP Contentuploads202208ExportFinalProgram 19082022113125 PDFMiguel AngelNo ratings yet
- UGC Journals List - 1Document232 pagesUGC Journals List - 1Amal Living MiracleNo ratings yet
- CV Paul Pronyk 2016Document3 pagesCV Paul Pronyk 2016Bobby Febri KrisdiyantoNo ratings yet
- DME Medical Billing Book 1662598386Document46 pagesDME Medical Billing Book 1662598386Nelson ANo ratings yet
- Drug Awareness CampaignDocument17 pagesDrug Awareness CampaignNicholas D. WolfwoodNo ratings yet
- An Observational Clinical Study of Association of Lintula Score in Suspected Case of Acute Appendicitis in Tertiary Care HospitalDocument5 pagesAn Observational Clinical Study of Association of Lintula Score in Suspected Case of Acute Appendicitis in Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Food Service and Pharmacy, LaundryDocument19 pagesFood Service and Pharmacy, LaundryRAGAVI BNo ratings yet
- Caring For Client When Death Is ImminentDocument23 pagesCaring For Client When Death Is ImminentNikki M. ArapolNo ratings yet
- Manejo y Control de Enfermedades RespiratoriasDocument13 pagesManejo y Control de Enfermedades RespiratoriasNicolás Ortiz RojasNo ratings yet
- Journal - A Review of Diabetes MellitusDocument6 pagesJournal - A Review of Diabetes Mellitusifaans16No ratings yet
- 412 Full PDFDocument61 pages412 Full PDFHarsya An-naafiahNo ratings yet
- A Care Study On BronchopneumoniaDocument35 pagesA Care Study On Bronchopneumoniaedna100% (1)
- Hap Vap Guidelines 2016 PDFDocument51 pagesHap Vap Guidelines 2016 PDFJerryEddyaPutraBoerNo ratings yet
- Endogenous Intoxication in SurgeryDocument5 pagesEndogenous Intoxication in SurgeryJonah Seeni100% (1)
- R Reeggaarrddiinngg Tthhee Eexxaam Miinnaattiioonn: GDD ? H@Qka A9Fk KMJ? GFK H9Cakl9FDocument3 pagesR Reeggaarrddiinngg Tthhee Eexxaam Miinnaattiioonn: GDD ? H@Qka A9Fk KMJ? GFK H9Cakl9FAamir HamaadNo ratings yet
- CLINICAL ToxicologyDocument29 pagesCLINICAL Toxicologykkrriissyy_0625No ratings yet
- HematuriaDocument32 pagesHematuriaSurya Nirmala DewiNo ratings yet
- Forensic Medicine NotesDocument8 pagesForensic Medicine NotesLloyd Anthony Valoria100% (1)
- SP 8Document2 pagesSP 8ray72roNo ratings yet
- Portal Hypertensive Gastropathy With A Focus On Management: ReviewDocument10 pagesPortal Hypertensive Gastropathy With A Focus On Management: ReviewDevy Widiya GrafitasariNo ratings yet
- Test Sas 16, 17 & 18 Nur 151 Cooa A4: Questions 1 To 10Document2 pagesTest Sas 16, 17 & 18 Nur 151 Cooa A4: Questions 1 To 10Sistine Rose LabajoNo ratings yet
- Npuap Epuap Pppia CPG 2017Document348 pagesNpuap Epuap Pppia CPG 2017RivanFirdausNo ratings yet
- BGL ChartDocument2 pagesBGL ChartJulie PearlNo ratings yet
- Casereport-Modified Radical MastectomyDocument33 pagesCasereport-Modified Radical MastectomyMayflor de LunaNo ratings yet