You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Viking ImpactDocument164 pagesThe Viking ImpactIkshkz Spplsp100% (4)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- TOPIC 1: Different Nautical ChartsDocument9 pagesTOPIC 1: Different Nautical ChartsRaymund Suaybaguio100% (2)
- Fragrance, Flavors and Food AdditivesDocument12 pagesFragrance, Flavors and Food AdditivesDaniel MalapitanNo ratings yet
- GBVDocument47 pagesGBVv_vijayakanth7656No ratings yet
- Loadings NSCP 2015 2 Storey Residential Concrete StructureDocument46 pagesLoadings NSCP 2015 2 Storey Residential Concrete StructureKenneth LauronNo ratings yet
- Geosynthetics in RailwaysDocument14 pagesGeosynthetics in RailwaysPrasanjit RoyNo ratings yet
- Chapter 10: Short-Term Financing and Intermediate-Term FinancingDocument17 pagesChapter 10: Short-Term Financing and Intermediate-Term FinancingHarold Dela FuenteNo ratings yet
- DBA 2.2 Ref SheetDocument2 pagesDBA 2.2 Ref SheetAxtklinge100% (1)
- HP 8904 Service ManualDocument137 pagesHP 8904 Service ManualWolverine Francesco TripaldiNo ratings yet
- Development MCQDocument4 pagesDevelopment MCQv_vijayakanth7656No ratings yet
- I Kick and I Fly by Ruchira GuptaDocument15 pagesI Kick and I Fly by Ruchira GuptaI Read YA100% (1)
- 3 PoshaDocument20 pages3 Poshav_vijayakanth7656No ratings yet
- Growing Up After Extremely Preterm Birth Lifespan Mental Health OutcomesDocument8 pagesGrowing Up After Extremely Preterm Birth Lifespan Mental Health Outcomesv_vijayakanth7656No ratings yet
- Functional Outcomes of Very Premature Infants Into AdulthoodDocument6 pagesFunctional Outcomes of Very Premature Infants Into Adulthoodv_vijayakanth7656No ratings yet
- Cerebral Palsy and Developmental Coordination Disorder in Children Born PretermDocument6 pagesCerebral Palsy and Developmental Coordination Disorder in Children Born Pretermv_vijayakanth7656No ratings yet
- Development 07HB29: Dominant 20Document2 pagesDevelopment 07HB29: Dominant 20v_vijayakanth7656No ratings yet
- Bone 1Document2 pagesBone 1v_vijayakanth7656No ratings yet
- V/Q and Oxygen: Anuja Abayadeera Part 1B AnaesthsiologyDocument42 pagesV/Q and Oxygen: Anuja Abayadeera Part 1B Anaesthsiologyv_vijayakanth7656No ratings yet
- Renal FailureDocument6 pagesRenal Failurev_vijayakanth7656No ratings yet
- Seminars in Pediatric Surgery Volume 21 Issue 1 2012 (Doi 10.1053/j.sempedsurg.2011.10.001) Robert C. Shamberger - Preface PDFDocument1 pageSeminars in Pediatric Surgery Volume 21 Issue 1 2012 (Doi 10.1053/j.sempedsurg.2011.10.001) Robert C. Shamberger - Preface PDFv_vijayakanth7656No ratings yet
- Fetal Macro So MiaDocument2 pagesFetal Macro So Miaapi-3712326No ratings yet
- Pediatrecs EmqDocument40 pagesPediatrecs Emqv_vijayakanth7656No ratings yet
- Age Group HT Cross TabulationDocument7 pagesAge Group HT Cross Tabulationv_vijayakanth7656No ratings yet
- Inferior Vena CavalDocument6 pagesInferior Vena Cavalv_vijayakanth7656No ratings yet
- Current Practice - Diabetic Ketoacidosis in ChildrenDocument10 pagesCurrent Practice - Diabetic Ketoacidosis in Childrenv_vijayakanth7656No ratings yet
- Ebola Virus DiseaseDocument4 pagesEbola Virus Diseasev_vijayakanth7656No ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument23 pagesChronic Obstructive Pulmonary Diseasev_vijayakanth7656No ratings yet
- Chronic Restrictive Lung DiseaseDocument20 pagesChronic Restrictive Lung Diseasev_vijayakanth7656No ratings yet
- St. Paul University SurigaoDocument3 pagesSt. Paul University SurigaoJoenetha Ann ApariciNo ratings yet
- Eco-Friendly Water FilterDocument2 pagesEco-Friendly Water FilterRaphael EdogunNo ratings yet
- 202010-02 Lowland WASH Weekly Reports PDFDocument24 pages202010-02 Lowland WASH Weekly Reports PDFAbebaw KebedeNo ratings yet
- May 032023Document7 pagesMay 032023Jannah MelonNo ratings yet
- Airfil Filters - Powered by Quality, Durability and ReliabilityDocument5 pagesAirfil Filters - Powered by Quality, Durability and ReliabilityMax SashikhinNo ratings yet
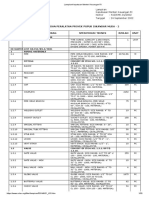
- LampiranKeputusan Menteri Keuangan RI Data PIM PDFDocument33 pagesLampiranKeputusan Menteri Keuangan RI Data PIM PDFkhomeinitjNo ratings yet
- VFD Pole Display PDFDocument48 pagesVFD Pole Display PDFdinil-udNo ratings yet
- Gabbett 2019 TheBig3Elements JOSPT InPressDocument9 pagesGabbett 2019 TheBig3Elements JOSPT InPressPrem AnandNo ratings yet
- Turtle Mountain Reservation by Louise Erdrich - Poetry FoundationDocument4 pagesTurtle Mountain Reservation by Louise Erdrich - Poetry Foundationdonna.w0736No ratings yet
- CG11 - 17 Preparation of Schedule of RatesDocument4 pagesCG11 - 17 Preparation of Schedule of RatesArdamitNo ratings yet
- SSADocument10 pagesSSAAnkush KumarNo ratings yet
- BLDV400Document60 pagesBLDV400Junaid SyedNo ratings yet
- Assignment 3Document5 pagesAssignment 3Ali Al RifaiNo ratings yet
- Principles For Layout Plans and Sectioning Diagrams For 25 KV Ac TractionDocument4 pagesPrinciples For Layout Plans and Sectioning Diagrams For 25 KV Ac TractionPragati SrivastavaNo ratings yet
- SOAL SEMESTER Genap KLS X 20202021 - Sastra InggrisDocument4 pagesSOAL SEMESTER Genap KLS X 20202021 - Sastra InggrisIka Endah MadyasariNo ratings yet
- Complaint Register 1Document79 pagesComplaint Register 1simon maaaklaNo ratings yet
- NOOK - Precision Screw AssembliesDocument216 pagesNOOK - Precision Screw AssembliesBruv 07No ratings yet
- Latihan Sas 1 Kelas 5 Bahasa InggrisDocument3 pagesLatihan Sas 1 Kelas 5 Bahasa InggrisLaila Purnamasari100% (1)
- A Rosenblatt Transformation Method Based On Copula Function For Solving Structural ReliabilityDocument7 pagesA Rosenblatt Transformation Method Based On Copula Function For Solving Structural ReliabilityRAJKUMAR SAHANo ratings yet
- Game Theory Problem SetDocument2 pagesGame Theory Problem SetChristian TanNo ratings yet
- Unidrive M Modular Drives v01 - 0 - 6Document75 pagesUnidrive M Modular Drives v01 - 0 - 6Dave CárdenasNo ratings yet