You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Agents of Edgewatch AP - Part 4 of 6 - Assault On Hunting Lodge Seven - Interactive Maps (PZPZO90160) PDFDocument5 pagesAgents of Edgewatch AP - Part 4 of 6 - Assault On Hunting Lodge Seven - Interactive Maps (PZPZO90160) PDFMuskratful MuskratNo ratings yet
- Chapter 10 - The Mature ErythrocyteDocument55 pagesChapter 10 - The Mature ErythrocyteSultan AlexandruNo ratings yet
- A Pictorial Guide For The Second Trimester Ultrasound: EducationDocument16 pagesA Pictorial Guide For The Second Trimester Ultrasound: EducationSultan AlexandruNo ratings yet
- APPENDIX A-Normal Values in HumansDocument22 pagesAPPENDIX A-Normal Values in HumansSultan AlexandruNo ratings yet
- Achieving Excellence in The OSCE Part 1Document409 pagesAchieving Excellence in The OSCE Part 1Sultan AlexandruNo ratings yet
- Cytopathology of Infectious DiseasesDocument404 pagesCytopathology of Infectious DiseasesSultan AlexandruNo ratings yet
- Achieving Excellence in The OSCE Part 2Document465 pagesAchieving Excellence in The OSCE Part 2Sultan AlexandruNo ratings yet
- MEDDICDocument5,328 pagesMEDDICSultan AlexandruNo ratings yet
- GI Practice Review - 2nd Edition - ABRThomson 2012Document744 pagesGI Practice Review - 2nd Edition - ABRThomson 2012Sultan AlexandruNo ratings yet
- APPENDIX B-Comparative HematologyDocument30 pagesAPPENDIX B-Comparative HematologySultan AlexandruNo ratings yet
- English ProficiencyDocument3 pagesEnglish ProficiencySultan AlexandruNo ratings yet
- Gepsych: Gepsych Productive Work OutputDocument1 pageGepsych: Gepsych Productive Work OutputCarlos ReyesNo ratings yet
- Cable Glands For Armoured and Non-Armoured CablesDocument6 pagesCable Glands For Armoured and Non-Armoured CablesmustardbassmanNo ratings yet
- 6SL3210 1PE11 8UL1 Datasheet enDocument2 pages6SL3210 1PE11 8UL1 Datasheet enMorris MorrisonNo ratings yet
- Vydyne® R533H NAT: Ascend Performance Materials Operations LLCDocument4 pagesVydyne® R533H NAT: Ascend Performance Materials Operations LLCJames FaunceNo ratings yet
- In The Name of Allah, The Merciful, The CompassionateDocument18 pagesIn The Name of Allah, The Merciful, The CompassionateShahzeb AlamNo ratings yet
- Chapter 11 QuestionsDocument4 pagesChapter 11 QuestionsEzechi Papaz UcheNo ratings yet
- AHAN End of Project Factsheet - ENGDocument2 pagesAHAN End of Project Factsheet - ENGNaughty VongNo ratings yet
- Joining Document Check List: Employee Code: Designation: Name: Department: LocationDocument1 pageJoining Document Check List: Employee Code: Designation: Name: Department: LocationNishi ojhaNo ratings yet
- Normas InternacionalesDocument3 pagesNormas Internacionalesmalota2108No ratings yet
- FBFV2 CodesDocument11 pagesFBFV2 CodesMa Ana Chinesa RedondoNo ratings yet
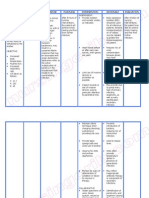
- Nursing Care Plan Neonatal SepsisDocument2 pagesNursing Care Plan Neonatal Sepsisderic100% (20)
- Data Analysis in Preclinical DevelopementDocument26 pagesData Analysis in Preclinical DevelopementOmkar KaleNo ratings yet
- 08 Handout 1Document7 pages08 Handout 1Cecille Marasigan AnzuresNo ratings yet
- RBI Grade B' Officer's Exam: Test-I General AwarenessDocument20 pagesRBI Grade B' Officer's Exam: Test-I General AwarenessShubhra TrivediNo ratings yet
- Organometallics 2005, 24, 3579-3581Document3 pagesOrganometallics 2005, 24, 3579-3581宋承恩No ratings yet
- Assaignment 1 GROUP B4Document9 pagesAssaignment 1 GROUP B4WinahyuNo ratings yet
- Instruction Sheet-ENG - SS - 408-32095 - B - 408-32095Document6 pagesInstruction Sheet-ENG - SS - 408-32095 - B - 408-32095MaxNo ratings yet
- Telma Butler: Intervention SpecialistDocument2 pagesTelma Butler: Intervention Specialistapi-301795519No ratings yet
- Learners Vaccination Inventory S.Y 2022 2023Document22 pagesLearners Vaccination Inventory S.Y 2022 2023CELIA T. BOLASTUGNo ratings yet
- 10 Contoh Teks Short 'Story Telling' Pendek Bahasa Inggris Unik Dan MenarikDocument13 pages10 Contoh Teks Short 'Story Telling' Pendek Bahasa Inggris Unik Dan MenarikDard TongNo ratings yet
- ZA20J Manuales de Operacion y SeguridadDocument104 pagesZA20J Manuales de Operacion y SeguridadNadia kristel Ayala escobarNo ratings yet
- Unsafe Areas at BoilerDocument2 pagesUnsafe Areas at BoilerPrabir PalNo ratings yet
- SlavicekDocument4 pagesSlavicekPAVLOSKONST0% (3)
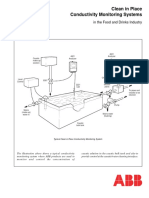
- Application Guide: Clean in Place Conductivity Monitoring SystemsDocument4 pagesApplication Guide: Clean in Place Conductivity Monitoring Systemspatitay036817No ratings yet
- Well Control Manual: Chapter 5 - Well Killing ProceduresDocument14 pagesWell Control Manual: Chapter 5 - Well Killing ProceduresMahrouz MadoNo ratings yet
- Hartnup Disease - Causes, Symptoms & DiagnosisDocument3 pagesHartnup Disease - Causes, Symptoms & DiagnosisYunistya Dwi Cahyani100% (1)
- Multiples Choice Questions With AnswersDocument60 pagesMultiples Choice Questions With AnswersVaibhav Rusia100% (2)
- Lecture 6 Streamflow Hydrograph Analysis Part (1-3)Document18 pagesLecture 6 Streamflow Hydrograph Analysis Part (1-3)Mahmoud AhmedNo ratings yet
- 2019 Sec 4 English SA1 St. Margaret's Secondary AnswerDocument10 pages2019 Sec 4 English SA1 St. Margaret's Secondary AnswerKairo ItsukiNo ratings yet