You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- PLC Programming With RSLogix 500Document132 pagesPLC Programming With RSLogix 500kemo_750252831No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- BS - 882Document12 pagesBS - 882Rifqi AnraNo ratings yet
- Safety Alarms Chiller and StarterDocument5 pagesSafety Alarms Chiller and StarterRaghavendra KaleNo ratings yet
- Pre Stressed Concrete Solved ProblemsDocument17 pagesPre Stressed Concrete Solved ProblemsJefferson T. Ignacio75% (28)
- Omnipeek GettingStartedDocument85 pagesOmnipeek GettingStartedchris100% (1)
- Failure Modes For Flooded & VRLA BatteriesDocument46 pagesFailure Modes For Flooded & VRLA Batteriesazhagaan100% (1)
- Shunt ResistorDocument7 pagesShunt ResistorAsghar AliNo ratings yet
- Training On Optical Fiber NetworkDocument96 pagesTraining On Optical Fiber Networkpriyasingh1682100% (1)
- Directional & Horizontal DrillingDocument23 pagesDirectional & Horizontal DrillingMuhammad shahbazNo ratings yet
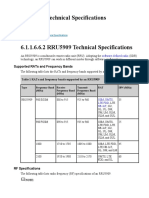
- RRU5909 Technical SpecificationsDocument7 pagesRRU5909 Technical SpecificationsDmitry059100% (1)
- Scalping Forex With Bollinger BandDocument27 pagesScalping Forex With Bollinger BandHeru SetiawanNo ratings yet
- Solids Induced Pack-Off Packing Off - First ActionsDocument4 pagesSolids Induced Pack-Off Packing Off - First ActionsBhagwal TravelsNo ratings yet
- Classification of Cerebral Arteriovenous Malformations and Intranidal Flow Patterns by Color-Encoded 4D-Hybrid-MRADocument8 pagesClassification of Cerebral Arteriovenous Malformations and Intranidal Flow Patterns by Color-Encoded 4D-Hybrid-MRARifqi AnraNo ratings yet
- 247 FullDocument8 pages247 FullRifqi AnraNo ratings yet
- Nidal Embolization of Brain Arteriovenous Malformations Using Onyx in 94 PatientsDocument6 pagesNidal Embolization of Brain Arteriovenous Malformations Using Onyx in 94 PatientsRifqi AnraNo ratings yet
- Outcome Analysis of Preoperative Embolization With N-Butyl Cyanoacrylate in Cerebral Arteriovenous MalformationsDocument7 pagesOutcome Analysis of Preoperative Embolization With N-Butyl Cyanoacrylate in Cerebral Arteriovenous MalformationsRifqi AnraNo ratings yet
- Preoperative Embolization of Cerebral Arteriovenous Malformations With OnyxDocument4 pagesPreoperative Embolization of Cerebral Arteriovenous Malformations With OnyxRifqi AnraNo ratings yet
- Arteriovenous Malformation of The Thyroid Gland As A Very Rare Cause of Mechanical Neck Syndrome: A Case ReportDocument6 pagesArteriovenous Malformation of The Thyroid Gland As A Very Rare Cause of Mechanical Neck Syndrome: A Case ReportRifqi AnraNo ratings yet
- Lampiran I: Setting Up Pengujian Di LaboratoriumDocument7 pagesLampiran I: Setting Up Pengujian Di LaboratoriumRifqi AnraNo ratings yet
- Takehome (Taufiq)Document234 pagesTakehome (Taufiq)Rifqi AnraNo ratings yet
- B. Perhitungan Kekakuan Elastis (K), P, P Dan Daktilitas BKN-2RDocument1 pageB. Perhitungan Kekakuan Elastis (K), P, P Dan Daktilitas BKN-2RRifqi AnraNo ratings yet
- Su Keystroke ShortcutsDocument2 pagesSu Keystroke ShortcutsRifqi AnraNo ratings yet
- Management LVDTDocument5 pagesManagement LVDTRifqi AnraNo ratings yet
- DEE APPLIED PHYSICS - Remedial TestDocument2 pagesDEE APPLIED PHYSICS - Remedial TestMilan SasmolNo ratings yet
- Newton First Law of MotionDocument6 pagesNewton First Law of MotionKin ChristineNo ratings yet
- Hypothesis Testing in Stata PDFDocument9 pagesHypothesis Testing in Stata PDFMarisela FuentesNo ratings yet
- Compacted Graphite Iron - Mechanical and Physical Properties For Engine DesignDocument22 pagesCompacted Graphite Iron - Mechanical and Physical Properties For Engine DesignThanhluan NguyenNo ratings yet
- Netway N4PS2037B CAT6 UTP Cable (Indoor)Document1 pageNetway N4PS2037B CAT6 UTP Cable (Indoor)Wearn Jian LaiNo ratings yet
- CADCAM PortfolioDocument5 pagesCADCAM PortfolioGuhan MNo ratings yet
- Warrick 26m Control de Nivel AuxiliarDocument3 pagesWarrick 26m Control de Nivel AuxiliarCarlos WayNo ratings yet
- KKC Model Number System2Document3 pagesKKC Model Number System2zayerirezaNo ratings yet
- Chapter 44 - Quarks, Leptons, and The Big BangDocument10 pagesChapter 44 - Quarks, Leptons, and The Big BangVV CepheiNo ratings yet
- Student Personal Prescriptive Path 2Document29 pagesStudent Personal Prescriptive Path 2api-377332228No ratings yet
- Eia Cea 608Document154 pagesEia Cea 608Максим РадионовNo ratings yet
- 9011 VW Rebar Strainmeter (E)Document2 pages9011 VW Rebar Strainmeter (E)JasonNo ratings yet
- Linear Motion4Document9 pagesLinear Motion4Jai GaizinNo ratings yet
- M.C.a.sem III Operation Research 1Document50 pagesM.C.a.sem III Operation Research 1Pankaj SatkarNo ratings yet
- Mark Scheme (Results) October 2020: Pearson Edexcel International Advanced Level in Core Mathematics C34 (WMA02) Paper 01Document29 pagesMark Scheme (Results) October 2020: Pearson Edexcel International Advanced Level in Core Mathematics C34 (WMA02) Paper 01nonNo ratings yet
- Diego 1Document22 pagesDiego 1acs_spNo ratings yet
- On Predicting Roller Milling Performance Part II. The Breakage FunctionDocument13 pagesOn Predicting Roller Milling Performance Part II. The Breakage FunctionKenneth AdamsNo ratings yet
- Sr. Grand Test Key and HintsDocument7 pagesSr. Grand Test Key and HintsM JEEVARATHNAM NAIDUNo ratings yet
- 3107 Enthusiast Score Advanced Paper-2 (E+H) JADocument56 pages3107 Enthusiast Score Advanced Paper-2 (E+H) JAsonu goyalNo ratings yet