You might also like
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- The Night FloorsDocument57 pagesThe Night FloorsNat LinkenNo ratings yet
- MediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Document2 pagesMediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Lhogeswaran RaviNo ratings yet
- 34 Ms Surgery LogbookDocument111 pages34 Ms Surgery LogbookMohamedHossam50% (2)
- Demand Forecasting QuestionsDocument30 pagesDemand Forecasting QuestionsgigipapasNo ratings yet
- Revision - The Existence of God and RevelationDocument51 pagesRevision - The Existence of God and RevelationnkznghidsnidvNo ratings yet
- Vera Pawlowsky-Glahn - Compositional Data Analysis in The Geosciences - From Theory To Practice-Geological Society (2006)Document214 pagesVera Pawlowsky-Glahn - Compositional Data Analysis in The Geosciences - From Theory To Practice-Geological Society (2006)javicol70No ratings yet
- Knet Open ERP ProposalDocument13 pagesKnet Open ERP ProposalRianov Aja100% (1)
- Mintel Global Consumer Trends 2030 April 2020 Shared by WorldLine TechnologyDocument48 pagesMintel Global Consumer Trends 2030 April 2020 Shared by WorldLine Technologylebaosip100% (1)
- NAIC Claim Form PDFDocument3 pagesNAIC Claim Form PDFMohit BaggaNo ratings yet
- National Inurance Company Limited - Claim FormDocument3 pagesNational Inurance Company Limited - Claim FormfuckyouprettyNo ratings yet
- 10 New India Assurance Company - Reimbursement Claim FormDocument3 pages10 New India Assurance Company - Reimbursement Claim FormbhurajeshNo ratings yet
- Fixed Claim FormDocument2 pagesFixed Claim FormVikas GiriNo ratings yet
- Claim FormDocument3 pagesClaim FormKhameer L Shah100% (1)
- The New India Assurance Company Limited: Claim NumberDocument3 pagesThe New India Assurance Company Limited: Claim Numberharshmanu1612No ratings yet
- 14) ELIB-Female CI-Claim FormDocument7 pages14) ELIB-Female CI-Claim Formbibianna93No ratings yet
- National Insurance Company LimitedDocument4 pagesNational Insurance Company Limitedkaransandesara777No ratings yet
- In-Patient Claim FormDocument2 pagesIn-Patient Claim Formfaisal_1241No ratings yet
- Claim FormDocument3 pagesClaim FormSumit ManglaniNo ratings yet
- Medical Claim Form (Reimbursement Only)Document2 pagesMedical Claim Form (Reimbursement Only)Muhammad Rizwan Tariq100% (1)
- Adamjee Insurance Company Limited: Health Insurance - In-Patient Claim FormDocument2 pagesAdamjee Insurance Company Limited: Health Insurance - In-Patient Claim FormubaidNo ratings yet
- NiramayaclaimformDocument2 pagesNiramayaclaimformu409023No ratings yet
- The Oriental Insurance Company Limited (Incorporated in India, Subsidiary of General Insurance Corporation of India)Document4 pagesThe Oriental Insurance Company Limited (Incorporated in India, Subsidiary of General Insurance Corporation of India)Mcnet WideNo ratings yet
- OIC Claim FormDocument4 pagesOIC Claim FormPrashant SinghNo ratings yet
- CFPA-Medical ExpensesDocument2 pagesCFPA-Medical ExpensesDivya VoletiNo ratings yet
- Claim Form NewDocument4 pagesClaim Form NewVicky GautamNo ratings yet
- Head Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.Document5 pagesHead Office: 87, M G Road, Fort, Mumbai-400001: I. II - CLAIM NO.gaddipati_ramuNo ratings yet
- Heritage Health - Pre Auth FormDocument6 pagesHeritage Health - Pre Auth FormBOOKREADER_NOWNo ratings yet
- Notification of Claim - Prudential GuaranteeDocument2 pagesNotification of Claim - Prudential GuaranteeZen Catolico ErumNo ratings yet
- Personal Statement Regarding HealthDocument5 pagesPersonal Statement Regarding HealthHarish ChandNo ratings yet
- Crewsure Claim Form (XLCatlin) 1.3Document2 pagesCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- Mediclaim FormDocument1 pageMediclaim Formpicrush2pmNo ratings yet
- Professional Indemnity DoctorsDocument3 pagesProfessional Indemnity DoctorskandulasbooksNo ratings yet
- 1582808855278-Reimbursement FormDocument14 pages1582808855278-Reimbursement FormSuresh MeenaNo ratings yet
- f5192 PDFDocument2 pagesf5192 PDFVishal AggawalNo ratings yet
- Certificate: (To Be Filled by The Hospital/ Nursing Home/ Clinic Authority)Document1 pageCertificate: (To Be Filled by The Hospital/ Nursing Home/ Clinic Authority)Darbha ShaliniNo ratings yet
- Personal Accident Claim FormDocument5 pagesPersonal Accident Claim FormMadhava Reddy MunagalaNo ratings yet
- Job Loss Claim FormDocument3 pagesJob Loss Claim FormAbdulkhadarJilani ShaikNo ratings yet
- Claim FormDocument5 pagesClaim Formsoumyadeep19478425No ratings yet
- Medical Reimbursement FormDocument2 pagesMedical Reimbursement FormMEMOONA ASHARNo ratings yet
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument4 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDeepakNo ratings yet
- UIICHdfc ClaimformDocument2 pagesUIICHdfc ClaimformdomyomglolNo ratings yet
- CLAIMS 008 1022 7 Certificate of ClaimantDocument3 pagesCLAIMS 008 1022 7 Certificate of ClaimantEmsNo ratings yet
- Attending Physicians Statement-Death ClaimDocument2 pagesAttending Physicians Statement-Death ClaimKen CelesteNo ratings yet
- ChecklistDocument9 pagesChecklistkarthikfuser0183No ratings yet
- Kolkata Claim Form - MD-IndiaDocument4 pagesKolkata Claim Form - MD-Indiadipankar0majumderNo ratings yet
- Details of Primary Insured: Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument5 pagesDetails of Primary Insured: Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ASumitThoratNo ratings yet
- InPatient Claim Form - Jubilee Life InsuranceDocument2 pagesInPatient Claim Form - Jubilee Life InsuranceJawad MuhammadNo ratings yet
- InPatient Claim Form - Jubilee Life InsuranceDocument2 pagesInPatient Claim Form - Jubilee Life InsuranceAhmad Zubair40% (5)
- Critical Illness Claim FormDocument23 pagesCritical Illness Claim FormHihiNo ratings yet
- Medical Performa UpdatedDocument4 pagesMedical Performa UpdatedTravel IndiaNo ratings yet
- Bajaj Allianz Cashless Request FormDocument3 pagesBajaj Allianz Cashless Request FormM/s MicrotechNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka: 4 T' Block, Jayanagar, Bangalore - 560 041Document3 pagesRajiv Gandhi University of Health Sciences, Karnataka: 4 T' Block, Jayanagar, Bangalore - 560 041BUVISANTHANo ratings yet
- Mdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormDocument5 pagesMdindia Healthcare Services (Tpa) Pvt. LTD.: Claim FormrhvenkatNo ratings yet
- Personal Accident Claim FormDocument1 pagePersonal Accident Claim FormAlvin Roddy0% (1)
- GMC Claim Form How To File A ClaimDocument4 pagesGMC Claim Form How To File A ClaimtweetknotNo ratings yet
- Application Med. Re-ImbDocument2 pagesApplication Med. Re-Imbzahid hussainNo ratings yet
- MAP Application Form (Rev20230719)Document3 pagesMAP Application Form (Rev20230719)Jen EugenioNo ratings yet
- Health Insurance Claim FormDocument3 pagesHealth Insurance Claim FormdivechahimanshuNo ratings yet
- P.I. Client Demand PackageDocument6 pagesP.I. Client Demand PackageDrew BallNo ratings yet
- Pre Authorization Form IHealthcareDocument2 pagesPre Authorization Form IHealthcarecooljack0850% (2)
- Inbound 6577992357115018748Document2 pagesInbound 6577992357115018748Sofia NacuaNo ratings yet
- Others Claim FormDocument5 pagesOthers Claim FormArvind RayNo ratings yet
- For Muli R Claim RJ Individ U FinalDocument1 pageFor Muli R Claim RJ Individ U FinalSuhendin SoehendinNo ratings yet
- PH IcformDocument4 pagesPH IcformHihiNo ratings yet
- Ac SequenceDocument4 pagesAc SequencejenolivaNo ratings yet
- SustainabilityDocument856 pagesSustainabilityErnest AcarNo ratings yet
- Performance TaskDocument2 pagesPerformance TaskElla RadaNo ratings yet
- SpeechDocument2 pagesSpeechAyu RiyuningNo ratings yet
- Keph205 PDFDocument18 pagesKeph205 PDFRohit Kumar YadavNo ratings yet
- PR ExamDocument6 pagesPR Exambernmarr100% (1)
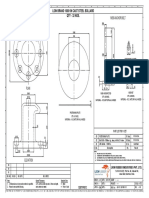
- M56 Anchor Bolt: Lion Brand 1000 KN Cast Steel Bollard Qty - 32 NosDocument1 pageM56 Anchor Bolt: Lion Brand 1000 KN Cast Steel Bollard Qty - 32 NossanaNo ratings yet
- Statistics in The Crem As of October 2020Document11 pagesStatistics in The Crem As of October 2020kamijou08No ratings yet
- Ford Ka Heater Fan Removal 1997 09Document3 pagesFord Ka Heater Fan Removal 1997 09Marius Dedal100% (1)
- Peritonitis NCPDocument3 pagesPeritonitis NCPANNA V. LARITANo ratings yet
- Math 237 p02 - Inexact de and Integrating Factors - 3172023-1Document18 pagesMath 237 p02 - Inexact de and Integrating Factors - 3172023-1Shunsui SyNo ratings yet
- Assignment 2 & 3 - PeaDocument3 pagesAssignment 2 & 3 - PeaShehzad khanNo ratings yet
- Intro. To EntrepreneurshipDocument20 pagesIntro. To EntrepreneurshipAnthonyNo ratings yet
- Solving For Discontinuities AlgebraicallyDocument22 pagesSolving For Discontinuities AlgebraicallyTuan HoangNo ratings yet
- God Created Integers PDFDocument3 pagesGod Created Integers PDFBryan0% (6)
- 16-4 I The Truth About Physician Health ProgramsDocument5 pages16-4 I The Truth About Physician Health ProgramslbandrewNo ratings yet
- Physics MCQs For Class 12 With Answers Chapter 10Document12 pagesPhysics MCQs For Class 12 With Answers Chapter 10Akshith ReddyNo ratings yet
- Syllabus FINA 6092 - Advanced Financial ManagementDocument5 pagesSyllabus FINA 6092 - Advanced Financial ManagementisabellelyyNo ratings yet
- Chemical Industry in China-FinalDocument48 pagesChemical Industry in China-Finalsandeep_scNo ratings yet
- Designreport Ner Roads Idg Sep19Document110 pagesDesignreport Ner Roads Idg Sep19yoseph dejeneNo ratings yet
- Answer Key-Averages ExerciseDocument3 pagesAnswer Key-Averages ExerciseVanshika WadhwaniNo ratings yet
- MDRM ReviewerDocument9 pagesMDRM Reviewerelsansebstian3506qcNo ratings yet
- Week 8 Perdev LasDocument8 pagesWeek 8 Perdev LasMay AnneNo ratings yet