You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Best Self-Defense - Training ModuleDocument28 pagesBest Self-Defense - Training ModuleNapoleon LygdasNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 12 Science of EmbodimentDocument5 pages12 Science of EmbodimentfelipeNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Kent's 12 ObservationsDocument4 pagesKent's 12 ObservationsRajesh Rajendran100% (4)
- Science DLP Form 2 Chapter 4 Human HealthDocument30 pagesScience DLP Form 2 Chapter 4 Human Healthseezack7976% (34)
- Respiratory Care Pocket Card English v2021.4 Pi58nnDocument2 pagesRespiratory Care Pocket Card English v2021.4 Pi58nnAdina BatajuNo ratings yet
- Form 2 Chapter 2Document7 pagesForm 2 Chapter 2naza977579% (19)
- EXAC Investor PresentationDocument21 pagesEXAC Investor PresentationmedtechyNo ratings yet
- Isuog USGDocument43 pagesIsuog USGflorenciaNo ratings yet
- IsomaltDocument22 pagesIsomaltPanneerselvam Dhanushkodi100% (1)
- Assignment On British American TobaccoDocument27 pagesAssignment On British American TobaccoAsad SaimonNo ratings yet
- Doctor's Kitchen 3-2-1: 3 Fruit and Veg, 2 Servings, 1 Pan - DR Rupy AujlaDocument5 pagesDoctor's Kitchen 3-2-1: 3 Fruit and Veg, 2 Servings, 1 Pan - DR Rupy Aujlarynykehi33% (3)
- What Is This Professor Freud Like - KoellreuterDocument140 pagesWhat Is This Professor Freud Like - KoellreuterJose MuñozNo ratings yet
- Introduction To PharmacologyDocument2 pagesIntroduction To PharmacologyJoy Ann Akia PasigonNo ratings yet
- Williams' Gynecology, Mcgraw-Hill, 2008 2. Berek, Jonathan S, Berek & Novak'S Gynecology, 14Th Edition, 2007Document1 pageWilliams' Gynecology, Mcgraw-Hill, 2008 2. Berek, Jonathan S, Berek & Novak'S Gynecology, 14Th Edition, 2007Nelly AstikaNo ratings yet
- Brain 2010 Missori Brain Awq014Document14 pagesBrain 2010 Missori Brain Awq014Nelly AstikaNo ratings yet
- HidrosefalusDocument10 pagesHidrosefalusNelly AstikaNo ratings yet
- Reproduction: A Comparative Analysis of The Zona Pellucida Birefringence of Fresh and Frozen-Thawed Human EmbryosDocument7 pagesReproduction: A Comparative Analysis of The Zona Pellucida Birefringence of Fresh and Frozen-Thawed Human EmbryosNelly AstikaNo ratings yet
- Function of The Acrosomal Matrix: Zona Pellucida 3 Receptor (ZP3R/sp56) Is Not Essential For Mouse FertilizationDocument17 pagesFunction of The Acrosomal Matrix: Zona Pellucida 3 Receptor (ZP3R/sp56) Is Not Essential For Mouse FertilizationNelly AstikaNo ratings yet
- Present As IDocument16 pagesPresent As INelly AstikaNo ratings yet
- Antepartum and Postpartum HemorrageDocument98 pagesAntepartum and Postpartum HemorrageNelly AstikaNo ratings yet
- HemorrhageDocument19 pagesHemorrhageNelly AstikaNo ratings yet
- Anatomic Disorders of Female Reproductive SystemDocument42 pagesAnatomic Disorders of Female Reproductive SystemNelly AstikaNo ratings yet
- Hemorrhage EeDocument7 pagesHemorrhage EeNelly AstikaNo ratings yet
- Hypothermic Treatment For Acute Spinal Cord Injury: ReviewDocument11 pagesHypothermic Treatment For Acute Spinal Cord Injury: ReviewNelly AstikaNo ratings yet
- Antepartum and Postpartum HemorrageDocument98 pagesAntepartum and Postpartum HemorrageNelly AstikaNo ratings yet
- Chapter 3 CaregiversDocument20 pagesChapter 3 CaregiversJuanNo ratings yet
- Fanny Nabiilah - 21040079 - Main Idea and Implied ExercisesDocument7 pagesFanny Nabiilah - 21040079 - Main Idea and Implied Exercisesbagas semNo ratings yet
- Ramadhan A. H. - Analyzing TextDocument6 pagesRamadhan A. H. - Analyzing TextRamadhan Abiyasa HariantoNo ratings yet
- NCM103 - Activity 1 PDFDocument2 pagesNCM103 - Activity 1 PDFFrancine Dominique CollantesNo ratings yet
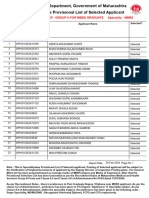
- MBBS Selected For WebsiteDocument195 pagesMBBS Selected For Websitemohaseen1112No ratings yet
- Dayrit. Ass 5. TFNDocument2 pagesDayrit. Ass 5. TFNDivine DayritNo ratings yet
- Perjeta Epar Product Information - enDocument43 pagesPerjeta Epar Product Information - enGeo GeoNo ratings yet
- Blood Bank Management System: Second PresentationDocument14 pagesBlood Bank Management System: Second Presentationsadaf hameedNo ratings yet
- Ophthalmology Referral Guidelines: Document IDDocument28 pagesOphthalmology Referral Guidelines: Document IDBambang AdiNo ratings yet
- Chapter14 Ob Physical and Physiological Changes During PregnancyDocument57 pagesChapter14 Ob Physical and Physiological Changes During Pregnancyth233No ratings yet
- ADocument3 pagesARita AnnaNo ratings yet
- ResumeDocument3 pagesResumeSean LoranNo ratings yet
- Concept Check 3 - JB PDFDocument2 pagesConcept Check 3 - JB PDFcdcdiver0% (1)
- Quarter 1-G7-CURMAP-TLE-23-24Document4 pagesQuarter 1-G7-CURMAP-TLE-23-24FSBTLED Nathan VinceNo ratings yet
- Laboratory and Diagnostic ExaminationDocument3 pagesLaboratory and Diagnostic ExaminationRose Anne MücklNo ratings yet
- Updated UNANG YAKAP CHECKLIST 1Document2 pagesUpdated UNANG YAKAP CHECKLIST 1ANGELYN TI-ADNo ratings yet
- Drugs On Reproductive System Physiology: N11 Pharmacology For NursesDocument2 pagesDrugs On Reproductive System Physiology: N11 Pharmacology For NursesAlec Xavier MirandaNo ratings yet