Sue, D. W. (1977). Community mental health services to
minority groups: Some optimism, some pessimist,
American Psychologist, 32(6), 616-624
Suc, D.W, (1992, Winter). The challenge of multiculturalism:
“The road less traveled, American Counselor, 1, 5-14
Sue, D.W. (1999, August). Multicultural competencies in the
profession of psychology. Symposium address delivered at
the 107th Annual Convention of the American Psycho-
logical Association, Boston,
Sue, D. W. (1999b, August). Surviving monoculturaisn and
racism A personal journey. Division 45. Presidential
Address delivered at the 107th Annual Convention of the
American Psychological Association, Boston,
Sue, D. W, Arredondo, P., & MeDaris, R. J. (1992), Muli
cultural counseling competencies and standards; A call
tothe profession. Journal of Counseling and Development,
70,477-486,
Sue, D. W,, 8 Sue, D. (2002), Counseling the culturally diverse:
‘Theory and practice (4th ed.) Hoboken, NJ: Wiley
Sullivan, C,, & Cottone, R, R, (2010). Emergent characteris:
tics of effective cross-cultural reseacch: A review of the
literature. Journal of Counseling & Development, 883),
357-362.
Summerfield, D. (1998). 4 critique of seven assumptions be-
hind psychological trauma programmes in war affected
areas, Socal Science and Medicine, $8, 1449-1462.
“Taylor, R, Chatters, L. M, 8 Levin, JS. 2008) Religion in
the lives of African Americans: Social, psychological, and
heath perspectives. Thousand Oaks, CA: Sage,
‘Taylor, SE. (2007). Social support. Ia H.$. Friedman &R.C.
Silver (Eds), Foundations of health psychology (pp. 45—
171), New York: Oxford University Press
‘Thompson, C, E., & Neville, H. A. (1999). Racism, mental
heath, and mental health practice. Coustseling Payckolo-
gist, 27, 155-223,
‘Trimble, J. B. (2007), Prolegomena for the connotation of
‘consiruct use in the measurement of ethnic and racial
ently. Journal of Cownseling Psychology, 54, 247-258,
US. Department of Health and Human Services, (2003). De
oleping cultural competence in disaster mental health pro
grams: Guiding principles ant recommendations. DHHS
Pub. No. SMA 3828, Rockville, MD: Center for Mental
Health Services, Substance Abuse and Mental Health Ser
vices Administration.
van den Eynde, J, & Veno, A. (1999). Coping with disastrous
‘events: An empowerment modal for community healing
In R Gist &B. Lubin (Eds), Response to disaster: Psycho-
social, community and ecological approaches (pp. 167—
192) Philadelphia: Brunnen/Mazel,
CHAPTER TWO Culturally Efective Helping 49
Weinrach, S. G. 2003, January). Letter: Mucb ado about
‘multiculturalism, part 4, Counseling Today, 45,31
Weinrach, S. G., & Thomas. KR, (1998). Diversity-sensitive
counseling today: A postmodern clash of values, Journal
of Counseling and Development, 76115122.
‘Weisaeth, L, (2000). Briefing and debriefing: Group psycho
logical interventions in acute stressor situations. In B.
Raphael & J. P. Wilson (Eds), Psychological debriefing
‘Theory, practice, and evidence (pp. 43-57). New York
Cambridge University Press
‘Whaley, A. L., & Davis, X. E. (2007). Cultural competence
and evidence-based practice in. mental health services.
American Psychologist, 62(6), 363-574
Williams, B, (2003). The worldview dimensions of tn-
dividualism and collectivism: Implications for
counseling. Journal of Counseling and Development,
8163), 370-372,
Winter, B, & Battle, L (2007, Mazch). Rolling sesslons: Squad
car therapy, Paper presented at Thirty-first Annual Con-
vening of Crisis Intervention Personnel and CONTACT
USA Conference, Chicago.
Worthington, R, L., & Dillion, FR. @01)), Deconstructing
‘multicultural counseling competencies research: Com-
ment on Oven, Leach, Wampold, and Rodolfa, Journal of
Counseling Psychology, $840), 10-15.
Worthington, R.L.. Sot-MCNett, A. M,,& Moreno, M, V,
(2007). Mutticulteral counseling competencies research
‘A 20-year content analysis. Journal of Counseling Psychol
24), 54, 39-36,
Wortman, C. B. & Lehman, D. R. (1985). Reactions to vie~
tims of life rises: Support attempts tha fall. In 1.G, Sara
son & B. R, Sarason (Eds), Socal support: Theory research
and application (pp. 483-488). Dordrecht, The Nether
Jands: Martinus Nijhodtf
‘Wubbolding, R.E, (2003, fenuary) Letters: Much ada about
‘mutticulturalisn, part 3. Cosseling Today, 45, 30-31.
Zalaquett, C., Carrion, [, & Exum, H, (2010). Providing di-
aster services to culturally diverse survivors. In Webber
& J.B. Mascasi (Eds), Terrorism, trauma ond tragedies:
A counselors guide to preparing and responding (rd ed,
pp. 19-24). Alexandria, VA: American Counseling Asso
lation Foundation
Zalaquett, C. P, Fuertb, K. M., Stein, C, Wey, A. Ey Selvey,
‘M. B. (2008). Reftaming the DSM-IV-R from a muiticul-
tural/social justice perspective. Journal of Counseling &
Development, 863), 364-371
Zimbethofl, A. K, & Brown, L. S, (2006). “Only the goyim
‘beat their wives, right” Paychology of Wonten Quarterly,
20, 422-424,
CHAPTER 3
The Intervention and
Assessment Models
Introduction
‘The purpose ofthis chapter isto present an applied cri-
‘sis intervention model that describes in detail the major
tasks involved in dealing witha crisis. The Triage As
sessment System i introduced as a rapid but systematic
technique for the crisis workee to use to adjudicate the
severity ofa client's presenting crisis situation and gain
some sense of direction in helping the client cope with
the dilemma. Finally, this chapter shares some ideas on
using referrals and gives some suggestions regarding
counseling difficult clients. This chapter and Chapter 4.
The Tools ofthe Trade, area prerequisite far succeeding
chapters, and we urge you to consider this foundation
material carefully
‘The model of crisis intervention you are about to
encounter emphasizes an immediacy mode of actively,
assertively, intentionally, and continuously assessing lis-
tening, and acting to systematically help the clint regain
as much peecrsis equiibeium, mobility, and autonomy
as possible. Two ofthose terms, equilibrium and mobility,
and their antonyms, disequilibrium and immobility, are
commonly used by crisis workers to identify client states
of being and coping. Because we will be using these
terms often, we would like to frst provide their diction-
ary definitions and then give a common analogy, so their
seaning becomes thoroughly understood,
Equilibrium. A state of mental or emotional stabil-
ity, balance, or poise in the organism.
Disequilibrium, Lack or destruction of emotional
stability, balance, or poise in the organism.
Mobility. A state of physical being in which the
person can autonomously change or cope in re-
sponse to different moods, feelings, emotions,
50
needs, conditions, influences; being flexible or
adaptable to the physical and social world
Immobility, A state of physical being in which the
person is not immediately capable of autono-
ously changing or coping in response to differ
ent moods, feelings, emotions, needs, conditions,
influences; inability to adapt to the immediate
physical and social world.
A healthy person is in a state of approximate psy-
chological and behavioral equilibrium, like a motorist
driving, with some starts and stops, down the road of
life—for both the short and the long haul. The person
‘ay hit some potholes but does not break any axles.
Aside from needing to give the car an occasional tune-
up, the person remains more or less equal to the task
‘of making the drive, In contrast, the person in cris
whether it be acute or chronic, is experiencing seviot
difficulty in steering and successfully navigating life's
highway. The individual is at least temporarily out of
control, unable to command personal resources or those
of others in order to stayon safe psychological pavement.
A healthy person is capable of negotiating hill
‘curves, ice, fog, stray animals, wrecks, and most other
‘obstacles that impede progress. No matter what road:
blocks may appear, such a person adapts to changing
conditions, applying brakes, putting on fog lights, and
estimating passing time. This person may have fender
benders from time to time butavoids head-on collisions.
‘The person in a dysfunctional state of equilibriam and
mobility has failed to pass inspection. Careening down
hills and around dangerous curves, knowing the brakes
have failed, the person is frozen with panic and despair
and has little hope of handling the perilous situation.
‘The result is that the person has become a victim of the
situation, has forgotten all about emergency brakes,
downshifting, or even easing the car into guardrails.
He or she flies headlong into catastrophe and watches
transfixed as it happens, The analogy of equilibrium
and mobility applies to most crisis situations. Thus, it
becomes every crisis worker's job to figuratively get the
client back into the driver's scat ofthe psychological ve-
hicle, As we shall see, sometimes this means the client
‘must temporarily leave the driving to us, sometimes it
‘means sitting alongside the client and pointing out the
rules of the road, and sometimes it means just pretty
‘much going along for the ride!
All of that being said, the crisis worker will mect a
number of individuals who were not poster children
for psychological equilibrium before the crisis. Many
people who were displaced by Hurricane Katrina, for
example, were physically and psychologically fragile
before the hurricane. We will have more to say about
such people, who are more typically in a state of
transcrisis, in Chapter 5, Crisis Case Handling
A Hybrid Model
of Crisis Intervention
Perhaps the biggest change in the seventh edition of
this book is our notion of how a model for crisis inter-
vention operates, There are numerous models for crisis
intervention (Aguilera, 1998; Kanel, 1999; Kleespies,
2009; Lester, 2002; Roberts, 2005; Slaikeu, 1990). All
of these models depict crisis intervention in some lin
car, stepwise fashion. Indeed, through 20-plus years of
publishing this book we did much the same, with the
admonition that changing conditions might well mean
that the interventionist would have to recycle and move
back to earlier steps. In our eatlier model we depicted
crisis intervention as starting with problem explora
tion, examining safety concerns, looking for support,
‘examining alternatives to present behaving, planning
how to restore equilibrium, and finally gaining a com-
mitment to take action, We no longer believe that a
stage or purely step model captures the way crisis inter-
vention works, and here's why.
‘The problem that we have struggled with as we try to
teach students like you about crisis intervention is that
at times crisis is anything but linear. lot of the times,
‘tisis intervention absolutely epitomizes chaos theory—
with starts, stops, do-overs, and U-turns. At times
doing crisis work is @ lat like being a smoke jumper,
CHAPTER THREE The Intervention and Assessment Models 51
controlling a psychological brush fire on ths side of the
mountain only to be faced with @ new one on the other
side of the valley. Fighting those psychological fires ac-
cording to a neat, progressive, linear plan is easly said
but not so easily done. Therefore, we have combined our
former linear model with a systems model we helped de-
velop (Myer, James, & Moulton, 2011), resulting in what
could more appropriately be called a hybrid model for
individual crisis intervention that is generally linear in
its progression but can also be seen in terms of tasks that,
need to be accomplished. While certainly some of these
tasks would usually be done in the beginning, middle,
‘or end of a crisis, changing conditions may mean yout
have to accomplish some task you would normally do
Inter, first, Or indeed, a task you thought was already
accomplished comes apart and has to be done over not
‘once, but raultiple times.
{A further problem with a strict linear model is that
each step should be discrete, following from step one to
step two and 90 on, with particular techniques to employ
in each of those steps. In crisis intervention, issues sud
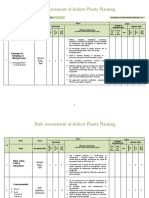
Iimayaitarcot
patonwioa- |Sootornueng |ayeereemenes [sceeret | Selah om
rotstcaton, | See Seesoset am |ehaowt end | Rater att |
wth ety minor onksion contusion sstoconsitusa. |
distortions. (Chent’s perception Client's perception | severe distortion
of realty, incuding |
Identity and describe bey the crs situation
Of crisis event may | paranoia, hat
Get insomere, | olcrsis event may | sie sussiaialy |uchallone and |
poate fom realty | afer natzaably | fomreamrar | Serene,
of stuation, from reaty ot | fom real creer ,
sation.
CRISIS EVENT
Se ete eee
AFFECTIVE DOMAIN
‘dentty and describe brielly the aft thats presont.
(iimore han one aifoet is experienced, rate with #1 being primary, #2 secondary, #3 tertiary)
ANGERIMOSTILITY
eee
FIGURE 2.2 (continued)
64 PARTONE Basie ‘rainings Crisis Intervention Theory and Application
CRISIS EVENT (continued)
ANXIETY FEAR,
‘SADNESSIMELANCHOLY.
FRUSTRATION,
BEHAVIORAL DOMAIN
Identity and deserite briety which behaviors curently being used.
(ifmera than ene behavir ie utized, rate wih #1 boing primary, #2 secondary, #3 tetany.)
APPROACH:
AVOIDANCE:
IMpAOILIT¥:
‘COGNITIVE DOMAIN
Idonity it ransgression, test, or loss has occured in he folowing areas and describe bile
(free than ono cognitive response occurs, rate with #1 Doing primary, #2 cecencary, # tariary)
PHYSICAL (lood, water, safety, shoe, et.)
Transgression _Threat__ Losa_
FSYCHOLOGIGAL (sel-concept, sense of emotional welktueing, ego Integy selFidenity, ee):
Transgression
‘SOCIAL RELATIONSHIPS {positive inleraction anc euppont, ‘amily end, coworkers, chuteh, clube, ete.
‘Threst___ Loss,
Transgression__Threst__ Loss
FIGURE 3.2 (continued)
CHAPTER THREE ‘the Intervention and Assessment Models 65
CRISIS EVENT (continued)
MORAL/SPIRITUAL (persona rtegiy, values, bait system, epi econeilation)
Peete eee Hee
Transgression _ Tweat___ Lose.
TRIAGE ASSESSMENT (x = Ital Ascossment / = Torna! Assessmen)
Feelings: Behaviors:
Anger___Fear__Sadness__ ‘Approech___Avcidanee__immobla_
— ——__
123456789 0 124456789 9
Thinking:
‘Wansgression___ Twweat____Loss.
123456789 0
Ina Total Scere: @X)__—
Terminal Total Score {0)__
[Describe the observations that led you to check the characteristics above
FIGURE 3.2 (continued)
The Affective Severity Scale. No crisis situa
tion that we know of has positive emotions attached
to it. Crow (1977) metaphorically names the ustal
emotional qualities found im a crisis as yellow (anxi-
ety), red (anger), and black (depression). To those we
would add orange (our students chose this color) for
frustration, which invariably occurs as clients attempt
to meet needs, These needs range all across Maslow's
needs hierarchy, from inability to get food, water, and
shelter (Hurricane Katrina) to interpersonal issues
(cttempts to regain boyfriendgirlfriend) to intraper-
sonal issues (get rid of the schizophrenic voices) to
spiritual concerns (God can't let this happen). Frus-
tration of needs is often the precursor of other nega
tive emotions, thoughts, and behaviors that plunge
the client further into crisis. Even more problematic,
some very famous psychologists have investigated
the relationship between frustration and aggression
and found that aggression is always a consequence of
frustration (Dollard et al., 1938, p. 1). That outcome
particularly does not bode well when the client is in
Undergirding these typical emotions may lie a can:
stellation of other negative emotions such as shame, be
trayal, humiliation, inadequacy, and horror (Collins &
Collins, 2005, pp. 25-26) Clients may manifest these
emotions both verbally and nonverbally, and the astute
crisis worker needs to be highly aware of incongruen-
You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Peri Quiz Board 219Document2 pagesPeri Quiz Board 219Melody Barredo50% (2)
- Comparison of Intraocular Pressure After Water Drinking Test in Primary Open Angle Glaucoma Patients Controlled With Latanoprost and TrabeculectomyDocument7 pagesComparison of Intraocular Pressure After Water Drinking Test in Primary Open Angle Glaucoma Patients Controlled With Latanoprost and TrabeculectomyDimas Djiwa DNo ratings yet
- Xcelera Brochure Updated (English)Document24 pagesXcelera Brochure Updated (English)Pablo Rosas100% (1)
- GWC - Company ProfileDocument4 pagesGWC - Company Profileelrajil100% (1)
- APSAC FI Guidelines 2012Document28 pagesAPSAC FI Guidelines 2012gdlo72No ratings yet
- Window Cleaning Safety GuidelineDocument4 pagesWindow Cleaning Safety Guidelinejhunvalencia1203No ratings yet
- Responsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFDocument64 pagesResponsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFPyae PyaeNo ratings yet
- Open Versus Closed Kinetic Chain Exercises For Patellofemoral Pain Syndrome - TsaiDocument44 pagesOpen Versus Closed Kinetic Chain Exercises For Patellofemoral Pain Syndrome - TsaiBaykal Çelik100% (1)
- UJA-Federation of New York Donor Recognition List 2022Document17 pagesUJA-Federation of New York Donor Recognition List 2022ericlkaplanNo ratings yet
- A Synopsis On: Consumer's Perception Towards Packaged Cold-Pressed Juices and Brand " PVT LTDDocument3 pagesA Synopsis On: Consumer's Perception Towards Packaged Cold-Pressed Juices and Brand " PVT LTDNationalinstituteDsnrNo ratings yet
- EMP Procedure in MalaysiaDocument24 pagesEMP Procedure in Malaysialamkinpark3373No ratings yet
- Vi. Nursing Care PlanDocument11 pagesVi. Nursing Care PlanSamantha BolanteNo ratings yet
- ARC 360 NGP InstructionManualDocument24 pagesARC 360 NGP InstructionManualLMTNo ratings yet
- Bajaj Allianz General Insurance Company LTD.: Declaration by The InsuredDocument1 pageBajaj Allianz General Insurance Company LTD.: Declaration by The InsuredArtiNo ratings yet
- Catheter WiresDocument56 pagesCatheter WiresSaud ShirwanNo ratings yet
- Winter Safety Toolbox TalkDocument18 pagesWinter Safety Toolbox TalkKristina100% (1)
- Iap Guidelines On Rickettsial Diseases in ChildrenDocument7 pagesIap Guidelines On Rickettsial Diseases in Childrenitaa19No ratings yet
- Ebook Electrocardiography For Healthcare Professionals PDF Full Chapter PDFDocument67 pagesEbook Electrocardiography For Healthcare Professionals PDF Full Chapter PDFkenneth.bell482100% (28)
- Alice in Michigan: A Financial Hardship StudyDocument58 pagesAlice in Michigan: A Financial Hardship StudydaneNo ratings yet
- Neurologic AssessmentDocument29 pagesNeurologic AssessmentJoessel_Marie__8991100% (1)
- Konsolidasi WelmiDocument72 pagesKonsolidasi WelmiWelmi Sulfatri IshakNo ratings yet
- Pengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseDocument9 pagesPengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseTjatur SurantullohNo ratings yet
- Dental Informatics PlusDocument1 pageDental Informatics PlusNagendra TyagiNo ratings yet
- AiepiDocument12 pagesAiepiRenzo Iván Marín DávalosNo ratings yet
- Feline Injection-Site Sarcoma - Todays Veterinary PracticeDocument12 pagesFeline Injection-Site Sarcoma - Todays Veterinary PracticeBla bla BlaNo ratings yet
- General Deductions (Under Section 80) : Basic Rules Governing Deductions Under Sections 80C To 80UDocument67 pagesGeneral Deductions (Under Section 80) : Basic Rules Governing Deductions Under Sections 80C To 80UVENKATESAN DNo ratings yet
- Developing Methodology For Evaluating The Ability of Indoor Materials To Support Microbial Growth Using Static Environmental ChambersDocument6 pagesDeveloping Methodology For Evaluating The Ability of Indoor Materials To Support Microbial Growth Using Static Environmental ChambersEugene GudimaNo ratings yet
- Postural DrainageDocument7 pagesPostural DrainagemohtishimNo ratings yet
- LENS Skin Disorders 2324Document49 pagesLENS Skin Disorders 2324Zyrille Moira MaddumaNo ratings yet