You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cash Payments Journal PDFDocument1 pageCash Payments Journal PDFMilena AckovicNo ratings yet
- F Inv 433Document1 pageF Inv 433alsone07No ratings yet
- Care Coordination: - Case Management - Disease ManagementDocument27 pagesCare Coordination: - Case Management - Disease Managementamarneh1969No ratings yet
- Medical DecisionDocument2 pagesMedical DecisioneduardodubonNo ratings yet
- IC One Page Financial Plan Template 9036 PDFDocument2 pagesIC One Page Financial Plan Template 9036 PDFrocky700inrNo ratings yet
- 0051 b825Document22 pages0051 b825krishnan1159No ratings yet
- Activos FijosDocument28 pagesActivos FijosArelyNo ratings yet
- Aruna Crab Meat Export To CanadaDocument12 pagesAruna Crab Meat Export To CanadaHendrikNo ratings yet
- Soal Latihan DDADocument1 pageSoal Latihan DDAMutia AzzahraNo ratings yet
- Account Usage and Recharge Statement From 02-May-2023 To 17-May-2023Document30 pagesAccount Usage and Recharge Statement From 02-May-2023 To 17-May-2023Arivazhagan RajendiranNo ratings yet
- Account Summary Portfolio Allocation: Brokerage Cash Balance Deposit Sweep Balance Total Securities Portfolio ValueDocument22 pagesAccount Summary Portfolio Allocation: Brokerage Cash Balance Deposit Sweep Balance Total Securities Portfolio ValueFerguson TchayaNo ratings yet
- Date: 16 Jun 2019 To,: (Please Quote This Reference Number in All Future Correspondence)Document2 pagesDate: 16 Jun 2019 To,: (Please Quote This Reference Number in All Future Correspondence)Sameer MandgeNo ratings yet
- Ekinops PM - Lc4-Mp2-A: 400G Line Module For ETS Compact ChassisDocument2 pagesEkinops PM - Lc4-Mp2-A: 400G Line Module For ETS Compact ChassisBhargav SomepalliNo ratings yet
- 1 Cost Volume Profit AnalysisDocument4 pages1 Cost Volume Profit AnalysisGreta BassettiNo ratings yet
- S4H - 894 Test ManagementDocument17 pagesS4H - 894 Test ManagementAlison MartinsNo ratings yet
- Blue and White Illustrated Medical Healthcare in The 21st Century Education Presentation - 20230925 - 110030 - 0000Document8 pagesBlue and White Illustrated Medical Healthcare in The 21st Century Education Presentation - 20230925 - 110030 - 0000Janix MagbanuaNo ratings yet
- T-Mobile Data Breach AssignmentDocument6 pagesT-Mobile Data Breach Assignmentrachana singhNo ratings yet
- Emerging Approach For Resource Over Provisioning: Presented by Venkadesh R 2023614033Document12 pagesEmerging Approach For Resource Over Provisioning: Presented by Venkadesh R 2023614033RUKESH KNo ratings yet
- An Introduction To Computer Networks - An Introduction To Computer Networks, Desktop Edition 2.0.10Document7 pagesAn Introduction To Computer Networks - An Introduction To Computer Networks, Desktop Edition 2.0.10Mike MikkelsenNo ratings yet
- TawarruqDocument5 pagesTawarruqOGETO WESLEYNo ratings yet
- JioMart Invoice 16491756280302451A 1Document2 pagesJioMart Invoice 16491756280302451A 1new nameNo ratings yet
- The Implementation of Ten Operation Management Decision in BusinessDocument32 pagesThe Implementation of Ten Operation Management Decision in BusinessNormyzatul AkmalNo ratings yet
- Csit 101 Assignment 1Document4 pagesCsit 101 Assignment 1api-266983757No ratings yet
- Account STMTDocument8 pagesAccount STMTvidhya vijayNo ratings yet
- AccountingDocument15 pagesAccountingRae Steven Saculo100% (1)
- Modern Logistics InfrastructureDocument52 pagesModern Logistics InfrastructureRuchita Rajani100% (1)
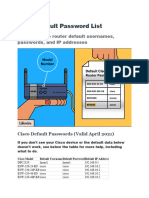
- Cisco Default Password ListDocument5 pagesCisco Default Password ListSiles Sandel100% (1)
- Chapter 02 - Rosenbloom 8edDocument28 pagesChapter 02 - Rosenbloom 8edAlyssa BasilioNo ratings yet
- The Accounting CycleDocument98 pagesThe Accounting CycleEhsan Sarparah100% (2)
- Lesson 3 Introduction To Bitcoin Block ChainDocument13 pagesLesson 3 Introduction To Bitcoin Block ChainVictor AjraebrillNo ratings yet