You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- TC18Document3 pagesTC18Robert BarnesNo ratings yet
- Lesson Plan HTNDocument14 pagesLesson Plan HTNGiri Siva87% (47)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Toefl PBT Test 3Document31 pagesToefl PBT Test 3Candra Gustika Sari50% (4)
- Pengetahuan, Sikap, Dan Perilaku Terhadap Pencegahan Serta Penanggulangan Hipertensi Di Kabupaten BogorDocument9 pagesPengetahuan, Sikap, Dan Perilaku Terhadap Pencegahan Serta Penanggulangan Hipertensi Di Kabupaten Bogorinna mayaNo ratings yet
- Celine SamanthaDocument2 pagesCeline SamanthaIRA ODETTE GATUSNo ratings yet
- Ada 2023Document294 pagesAda 2023Ahmed Ashab FerdousNo ratings yet
- Psychosomatic Disorders 22-1-2010Document36 pagesPsychosomatic Disorders 22-1-2010Raja174No ratings yet
- Black and White Race Differences in Aerobic Capacity, Muscle Fiber Type, and Influence On Metabolic Processes.Document9 pagesBlack and White Race Differences in Aerobic Capacity, Muscle Fiber Type, and Influence On Metabolic Processes.李博No ratings yet
- JNC 8 Versus JNC 7 - Understanding The Evidences: Research ArticleDocument6 pagesJNC 8 Versus JNC 7 - Understanding The Evidences: Research Articlemol3yNo ratings yet
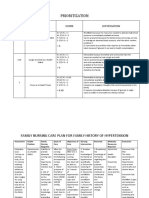
- Family Nursing Care Plan HypertensionDocument4 pagesFamily Nursing Care Plan HypertensionDarlene Joy AquinoNo ratings yet
- Midterm NotesDocument28 pagesMidterm NotesGen FranchesKyle Cortez ErigbuagasNo ratings yet
- Reviewer #1 (Sir Labajo)Document10 pagesReviewer #1 (Sir Labajo)Marivy GalonNo ratings yet
- Pharmacology - Drug Cards (Index Cards)Document272 pagesPharmacology - Drug Cards (Index Cards)Henrietta100% (9)
- Pcol MidtermsDocument25 pagesPcol MidtermsnoyaNo ratings yet
- Quick ReminderDocument13 pagesQuick RemindersindhuravemuNo ratings yet
- Dietary Management NephritisDocument29 pagesDietary Management Nephritisssbiswal42No ratings yet
- Preparation and Characterisation of Torsemide MicrocapsulesDocument9 pagesPreparation and Characterisation of Torsemide MicrocapsulesBaru Chandrasekhar RaoNo ratings yet
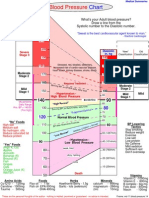
- Blood Pressure ChartDocument1 pageBlood Pressure ChartKAKKAMPI94% (16)
- Sutanon 250Document7 pagesSutanon 250dedyNo ratings yet
- The Prefrontal Cortex and Obesity A Health Neuroscience PerspectiveDocument13 pagesThe Prefrontal Cortex and Obesity A Health Neuroscience PerspectiveIgnacio DuqueNo ratings yet
- OET Letter Format 1 1Document6 pagesOET Letter Format 1 1MahmoudSelim100% (1)
- Seminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicDocument17 pagesSeminar: Kamyar Kalantar-Zadeh, Tazeen H Jafar, Dorothea Nitsch, Brendon L Neuen, Vlado PerkovicJack JackNo ratings yet
- Carboprost Drug StudyDocument3 pagesCarboprost Drug StudyAjay SupanNo ratings yet
- Cardiac Disease in PregnancyDocument5 pagesCardiac Disease in PregnancyArely GomezNo ratings yet
- Stress Management.Document404 pagesStress Management.James Adhikaram100% (1)
- Health History 3Document2 pagesHealth History 3boinkjilijoyNo ratings yet
- Product Manual ChronicDocument56 pagesProduct Manual ChronicsubhojitnayekNo ratings yet
- BSA Medical Form 680-001 A, B, C - 2014 PrintingDocument4 pagesBSA Medical Form 680-001 A, B, C - 2014 PrintingSarah Lowery FernandezNo ratings yet
- Mid A AssignmentDocument24 pagesMid A AssignmentTHE HOWDAY COMPANYNo ratings yet
- TS Report en WebdownloadDocument175 pagesTS Report en WebdownloadMartin NardoNo ratings yet