You might also like
- Urine Analysis PracticalDocument53 pagesUrine Analysis PracticalMubasharAbrar100% (3)
- Urinary Tract Disorders, PowerpointDocument63 pagesUrinary Tract Disorders, Powerpointmutia mutia100% (4)
- AMSEP Application FormDocument4 pagesAMSEP Application Formjayen_98No ratings yet
- Urine Analysis: Sbmitted To:dr - Jayganeesh Asst - Professor Dept - of Modern Diagnosis Submitted By:manisha Nandan 3 Year BNYSDocument30 pagesUrine Analysis: Sbmitted To:dr - Jayganeesh Asst - Professor Dept - of Modern Diagnosis Submitted By:manisha Nandan 3 Year BNYSMeera NandanNo ratings yet
- Nursing Foundation: Mrs. Neha Babru Asst - ProfessorDocument29 pagesNursing Foundation: Mrs. Neha Babru Asst - ProfessorSharon LawrenceNo ratings yet
- 50, 51. Diseases of The Equine Urinary TractDocument20 pages50, 51. Diseases of The Equine Urinary TractNatalie HowardNo ratings yet
- Physical Characteristics of UrineDocument36 pagesPhysical Characteristics of Urinemuhammad saad100% (1)
- Urinalysis 150313040235 Conversion Gate01Document30 pagesUrinalysis 150313040235 Conversion Gate01AbhishiktaAbhi100% (1)
- Lab 9++10 Pathological UrinlysisDocument38 pagesLab 9++10 Pathological UrinlysisSai SreedharNo ratings yet
- Urine-Analysis 140420Document74 pagesUrine-Analysis 140420sabao kizuiteNo ratings yet
- Urinalysis and Other Diagnostic Modalities in Nephrology MD3Document76 pagesUrinalysis and Other Diagnostic Modalities in Nephrology MD3juliuskahabi1No ratings yet
- UrinalysisDocument61 pagesUrinalysisMohammed AyaleqNo ratings yet
- Pbl-Gin Urine Test (Feme)Document11 pagesPbl-Gin Urine Test (Feme)KarthigaRamanNo ratings yet
- Urine Analysis FinalDocument112 pagesUrine Analysis FinalNischita JayarajNo ratings yet
- Urine Examination# DivyaDocument69 pagesUrine Examination# DivyaMedicine 0786No ratings yet
- Chemical Examination of UrineDocument32 pagesChemical Examination of UrineMarti DeaneNo ratings yet
- Urinalysis PDFDocument56 pagesUrinalysis PDFTio AjhaNo ratings yet
- 4 - Urine BenchDocument37 pages4 - Urine BenchChiizu iraNo ratings yet
- Urine Analysis: Dr. Janani MathialaganDocument67 pagesUrine Analysis: Dr. Janani MathialaganGunjan sahuNo ratings yet
- Genito Urinary TractDocument199 pagesGenito Urinary TractKim GonzalesNo ratings yet
- Urine Sediment Examination PDFDocument66 pagesUrine Sediment Examination PDFDapot SianiparNo ratings yet
- Urine AnalysisDocument41 pagesUrine AnalysisAjay SomeshwarNo ratings yet
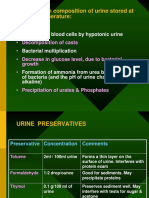
- Changes in Composition of Urine Stored at Room TemperatureDocument39 pagesChanges in Composition of Urine Stored at Room TemperatureAjay SomeshwarNo ratings yet
- Renal Function Test Amcj 8Document42 pagesRenal Function Test Amcj 8Md. Saifur Rahman SunnyNo ratings yet
- UrinalysisDocument12 pagesUrinalysisNamrah SyedNo ratings yet
- URINALYSISDocument80 pagesURINALYSISredr7131No ratings yet
- Urine AnalysisDocument42 pagesUrine AnalysisajaysomNo ratings yet
- Formation of Urine: NephronDocument44 pagesFormation of Urine: NephronajaysomNo ratings yet
- Renal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesDocument44 pagesRenal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesajaysomNo ratings yet
- Abnormal Constituents of Urine Interpretation PracticalDocument42 pagesAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiNo ratings yet
- Genito-Urinary Tract Disorders By: Mtespiriturnmd: NephronDocument10 pagesGenito-Urinary Tract Disorders By: Mtespiriturnmd: NephronCristybaby MunozNo ratings yet
- Color, PH and Specific GravityDocument19 pagesColor, PH and Specific GravityWilliam CapaciteNo ratings yet
- Week 3 Renal DisorderDocument74 pagesWeek 3 Renal DisorderManal jNo ratings yet
- 1 - GueDocument24 pages1 - GueQasmNo ratings yet
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument45 pagesGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomNo ratings yet
- UrinalysisDocument120 pagesUrinalysisKate Alyssa Caton100% (1)
- By: Dr. Yoavita Moderator: Dr. Anik Widijanti, SP - PK (K)Document61 pagesBy: Dr. Yoavita Moderator: Dr. Anik Widijanti, SP - PK (K)Gilang KusdinarNo ratings yet
- Urine ExaminationDocument45 pagesUrine ExaminationSalwa FaisalNo ratings yet
- Stool ExaminationDocument93 pagesStool ExaminationWajid SultanNo ratings yet
- Urinalysis: Finding The Clues Hidden in UrineDocument13 pagesUrinalysis: Finding The Clues Hidden in UrineIrvanNo ratings yet
- 3.4.5.A UrinalysisDocument13 pages3.4.5.A UrinalysisSadam Hussain JokhioNo ratings yet
- Urine AnalysisDocument33 pagesUrine AnalysisajaysomNo ratings yet
- Acute Renal Failure SymptomsDocument10 pagesAcute Renal Failure SymptomsEdwin Delos Reyes AbuNo ratings yet
- Urinalysis - Fatin AinaDocument14 pagesUrinalysis - Fatin AinaAl- ImanuddinNo ratings yet
- MED2 2022 (Autosaved)Document33 pagesMED2 2022 (Autosaved)Adakun SamuelNo ratings yet
- 2.physical ch. urine د.هناديDocument22 pages2.physical ch. urine د.هناديAbdulmalik Al-harthyNo ratings yet
- MLS 214 Physical Examination 2020Document34 pagesMLS 214 Physical Examination 2020Nabaa AlneshaimiNo ratings yet
- Clinical Analytical MethodsDocument47 pagesClinical Analytical MethodsDesta Yakob Doda 18BML0121No ratings yet
- Urine AnalysisDocument63 pagesUrine AnalysisVench DemicaisNo ratings yet
- Urinalysis PDFDocument34 pagesUrinalysis PDFAzeli SiquianNo ratings yet
- Urine AnalysisDocument31 pagesUrine AnalysisajaysomNo ratings yet
- Urinalysis PresentationDocument32 pagesUrinalysis PresentationMohamed SaadNo ratings yet
- Urine AnalysisDocument28 pagesUrine Analysisomatre210No ratings yet
- Odour: Physical ExaminationDocument27 pagesOdour: Physical ExaminationajaysomNo ratings yet
- Urine AnalysisDocument53 pagesUrine AnalysisMaath KhalidNo ratings yet
- Basic Examination of The Urine Specimen: Mr. Zumbeng Solomon Atebubu Municipal Hospital LaboratoryDocument65 pagesBasic Examination of The Urine Specimen: Mr. Zumbeng Solomon Atebubu Municipal Hospital LaboratoryAbdul-Rauf Suley MohammedNo ratings yet
- Exam 6 NotesDocument17 pagesExam 6 NotesWhitney WilliamsNo ratings yet
- Urine ComponentsDocument31 pagesUrine ComponentsLarry MagwegweNo ratings yet
- Laboratory Safety: Ann Fatima G. Quindao, RMT, LPT, MPHDocument43 pagesLaboratory Safety: Ann Fatima G. Quindao, RMT, LPT, MPHJanelou PalenNo ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisRating: 3 out of 5 stars3/5 (1)
- Brosur Penyuluhan Gizi Anak SekolahDocument2 pagesBrosur Penyuluhan Gizi Anak SekolahTia AriantiNo ratings yet
- Penyakit Jantung HipertensiDocument24 pagesPenyakit Jantung HipertensiTia AriantiNo ratings yet
- Jurnal 1Document13 pagesJurnal 1Tia AriantiNo ratings yet
- Soal Ujian EkgDocument12 pagesSoal Ujian EkgTia AriantiNo ratings yet
- Fatty Liver - HandoutDocument31 pagesFatty Liver - HandoutTia AriantiNo ratings yet
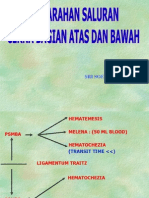
- Perdarahan Saluran Cerna Atas Dan BawahDocument24 pagesPerdarahan Saluran Cerna Atas Dan BawahTia AriantiNo ratings yet
- Perdarahan Saluran Cerna Atas Dan BawahDocument34 pagesPerdarahan Saluran Cerna Atas Dan BawahTia AriantiNo ratings yet
- Congestive Heart Failure CHF: Nik Nikam, M.DDocument94 pagesCongestive Heart Failure CHF: Nik Nikam, M.DTia AriantiNo ratings yet
- Chapter 9 Urinary System: Lesson 1Document23 pagesChapter 9 Urinary System: Lesson 1Tia AriantiNo ratings yet
- Robbery With Violence of Intimidation of Persons: BearodDocument6 pagesRobbery With Violence of Intimidation of Persons: BearodIsabella RodriguezNo ratings yet
- Nurse Educator ResumeDocument1 pageNurse Educator Resumeapi-643881078No ratings yet
- Class V Cavity Preparation For Amaglam Indications: 1-CariesDocument6 pagesClass V Cavity Preparation For Amaglam Indications: 1-CariesSamer AlRefaayNo ratings yet
- Q4-PPT-PE10 - Lesson 2 (Dance Forms Elements and Techniques)Document28 pagesQ4-PPT-PE10 - Lesson 2 (Dance Forms Elements and Techniques)Judy Ann FunitNo ratings yet
- Session 2-3Document33 pagesSession 2-3KANIKA GORAYANo ratings yet
- FSD Kenya Prequalification 2023 2026 ProjectsDocument7 pagesFSD Kenya Prequalification 2023 2026 ProjectsSolomon MainaNo ratings yet
- Ophtha Quiz - Lens Anatomy & Type of CataractDocument3 pagesOphtha Quiz - Lens Anatomy & Type of CataractAsif MohammedNo ratings yet
- BSBOPS502 Training PlanDocument13 pagesBSBOPS502 Training PlanMuhammad Zainal AbidinNo ratings yet
- Jlqzor: Sacred HealingDocument162 pagesJlqzor: Sacred HealingGuille monsterNo ratings yet
- Safety Data Sheet: Pt. Musim MasDocument6 pagesSafety Data Sheet: Pt. Musim MasfNo ratings yet
- International Personality Disorder Examiniation IPDEDocument5 pagesInternational Personality Disorder Examiniation IPDEbaralanu93No ratings yet
- LESSON PLAN - Peptic Ulcer - MDDocument11 pagesLESSON PLAN - Peptic Ulcer - MDmohamad dildar100% (3)
- A Comparative Study of Behavioural Pattern in Children of 5-15 Years of Age in Single Child Vs Child With SiblingsDocument5 pagesA Comparative Study of Behavioural Pattern in Children of 5-15 Years of Age in Single Child Vs Child With SiblingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Keravita ProDocument3 pagesKeravita ProNorman StoneNo ratings yet
- Method of Statement - Night Works - FINAL - 17092021Document17 pagesMethod of Statement - Night Works - FINAL - 17092021Syazwan ImanNo ratings yet
- Activity Worksheet No.3 Tle 7Document13 pagesActivity Worksheet No.3 Tle 7Jeanne Pauline Oabel100% (1)
- West Bengal State University: Cbcs Sem-Vi Examination, 2023 Regular CandidateDocument1 pageWest Bengal State University: Cbcs Sem-Vi Examination, 2023 Regular Candidatenandinirou5No ratings yet
- Ind 6 - Health Part 1 of 2 Jan 18 2021Document17 pagesInd 6 - Health Part 1 of 2 Jan 18 2021virupakshaNo ratings yet
- (Interactive Digital) S3 My CCE Journal - Updated 2 Nov 22Document24 pages(Interactive Digital) S3 My CCE Journal - Updated 2 Nov 22Irfan RaziqNo ratings yet
- EEG Sleep StagingDocument5 pagesEEG Sleep StagingIstiaqAnsariRakibNo ratings yet
- Session #41 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Document5 pagesSession #41 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- Lesson1structureandfunction Circulatorysystem 140718072518 Phpapp01Document45 pagesLesson1structureandfunction Circulatorysystem 140718072518 Phpapp01Richel Escalante MaglunsodNo ratings yet
- Contoh SURVEY GIZIDocument12 pagesContoh SURVEY GIZINandya AgustinaNo ratings yet
- Johnson & Johnson: Caring For People, Worldwide: Nilanjan Sengupta & Mousumi SenguptaDocument40 pagesJohnson & Johnson: Caring For People, Worldwide: Nilanjan Sengupta & Mousumi SenguptaRaavananNo ratings yet
- 30-Minute English TestDocument1 page30-Minute English TestLệ LưuNo ratings yet
- PHCG Ethiopia Overview PresentationDocument25 pagesPHCG Ethiopia Overview PresentationEyob MekonnenNo ratings yet
- Virex®II 256: One-Step Disinfectant Cleaner and DeodorantDocument2 pagesVirex®II 256: One-Step Disinfectant Cleaner and DeodorantPriyankhaNo ratings yet
- Improving Emotional Intelligence (EQ)Document7 pagesImproving Emotional Intelligence (EQ)Iuli IuliusNo ratings yet
- Emilio Aguinaldo College Nursing Care PlanDocument1 pageEmilio Aguinaldo College Nursing Care Planamal abdulrahmanNo ratings yet