You might also like
- ISS TCSTrngManualT0012E PDFDocument334 pagesISS TCSTrngManualT0012E PDFCharlie BarberNo ratings yet
- BS en 01672-1-2014Document60 pagesBS en 01672-1-2014Valeriy Golovin100% (1)
- ST FRANCIS of ASSISI, PETRUS ROMANUS, HILTON PETER MIJOVICK, NWO, NESARA, SCAMDocument325 pagesST FRANCIS of ASSISI, PETRUS ROMANUS, HILTON PETER MIJOVICK, NWO, NESARA, SCAMvampirebbqNo ratings yet
- Lift Curve SlopeDocument52 pagesLift Curve SlopeAISHWARYA GOLEYNo ratings yet
- Efficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialDocument5 pagesEfficacy of Micronised Vaginal Progesterone Versus Oral Dydrogestrone in The Treatment of Irregular Dysfunctional Uterine Bleeding: A Pilot Randomised Controlled TrialAna Di JayaNo ratings yet
- Effectiveness of Homoeopathy in The Cases of Verruca Vulgaris With The Aid of Complete Repertory - A Randomized, Single Blind Control TrialDocument6 pagesEffectiveness of Homoeopathy in The Cases of Verruca Vulgaris With The Aid of Complete Repertory - A Randomized, Single Blind Control TrialAnonymous CwJeBCAXpNo ratings yet
- Multivitamin and Micronutrient TreatmentDocument7 pagesMultivitamin and Micronutrient Treatmentanand809No ratings yet
- Single Dose of Fosfomycin Trometamol Versus Five Days Norfloxacin in The Treatment of Lower Uncomplicated Urinary Tract InfectionsDocument5 pagesSingle Dose of Fosfomycin Trometamol Versus Five Days Norfloxacin in The Treatment of Lower Uncomplicated Urinary Tract InfectionsIOSRjournalNo ratings yet
- Ureaplasma Urealyticum and Ureaplasma Parvum in Women of Reproductive AgeDocument17 pagesUreaplasma Urealyticum and Ureaplasma Parvum in Women of Reproductive AgeVivek mandalNo ratings yet
- 1 s2.0 S0377123714001567 MainDocument4 pages1 s2.0 S0377123714001567 MainMuhammad AzkaNo ratings yet
- AddyzoaDocument16 pagesAddyzoajackofmanytradesNo ratings yet
- ContentServer - Asp 13Document7 pagesContentServer - Asp 13Fitria NurulfathNo ratings yet
- Tmp117e TMPDocument6 pagesTmp117e TMPFrontiersNo ratings yet
- January 2003: East African Medical Journal 51Document5 pagesJanuary 2003: East African Medical Journal 51simoncktNo ratings yet
- Singh. NMP Better Result VS DYDDocument2 pagesSingh. NMP Better Result VS DYDRuth RachmawatyNo ratings yet
- 2008 AnnualDocument100 pages2008 AnnualKori PratiwiNo ratings yet
- Low-Dose Mifepristone in Treatment of Uterine Leiomyoma: A Randomised Double-Blind Placebo-Controlled Clinical TrialDocument8 pagesLow-Dose Mifepristone in Treatment of Uterine Leiomyoma: A Randomised Double-Blind Placebo-Controlled Clinical TrialAlrick GonzalezNo ratings yet
- Ustekinumab Psoriasis SingaporeDocument14 pagesUstekinumab Psoriasis SingaporeCHONG WEI SHENGNo ratings yet
- Tele The Ruthr AbotuDocument5 pagesTele The Ruthr AbotukhanjanNo ratings yet
- A Comparison Between Epidural and IV Tramadol For Painless Labor and Effect On Perinatal OutcomeDocument10 pagesA Comparison Between Epidural and IV Tramadol For Painless Labor and Effect On Perinatal OutcomeLibay Villamor IsmaelNo ratings yet
- MR 20 45301Document6 pagesMR 20 45301MOSTOFA SHAMIM FERDOUSNo ratings yet
- Pediatric Pharmacotherapy: CefipimeDocument9 pagesPediatric Pharmacotherapy: Cefipimeashfaq ahmedNo ratings yet
- Comparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialDocument5 pagesComparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialVindee VictoryNo ratings yet
- Antimalarial Potential of Nosode 30 and 200 Against Plasmodium Berghei Infection in BALB/c MiceDocument6 pagesAntimalarial Potential of Nosode 30 and 200 Against Plasmodium Berghei Infection in BALB/c MiceDexter BluesNo ratings yet
- Joc 911151Document8 pagesJoc 911151Daniel BorgesNo ratings yet
- Oral Spironolactone For Acne Vulgaris in Adult Females: Dr. Sami AlshakhashirDocument20 pagesOral Spironolactone For Acne Vulgaris in Adult Females: Dr. Sami AlshakhashirMazen DahshanNo ratings yet
- The Pharmacodynamics and Pharmacokinetics of Mivacurium in ChildrenDocument7 pagesThe Pharmacodynamics and Pharmacokinetics of Mivacurium in ChildrenluyawinNo ratings yet
- Association Between Asymptomatic Bacteriuria and Pre-Eclampsia.Document5 pagesAssociation Between Asymptomatic Bacteriuria and Pre-Eclampsia.alfiahNo ratings yet
- Effectiveness of High-Dose Glucocorticoids On Hemolysis, Elevating Liver Enzymes, and Reducing Platelets SyndromeDocument10 pagesEffectiveness of High-Dose Glucocorticoids On Hemolysis, Elevating Liver Enzymes, and Reducing Platelets SyndromeAlfa FebriandaNo ratings yet
- Amh Serum Dan CairanDocument2 pagesAmh Serum Dan CairanAnton ArifinNo ratings yet
- Aub PDFDocument3 pagesAub PDFNinikNo ratings yet
- Obstetric and Gynecology JournalDocument3 pagesObstetric and Gynecology JournalSiti AlfianaNo ratings yet
- Delamanid For MDR TB (Journal Reading)Document20 pagesDelamanid For MDR TB (Journal Reading)Gede Ngurah ProboNo ratings yet
- 33 - 4 - 07-Dr - KhademDocument5 pages33 - 4 - 07-Dr - Khademedy744No ratings yet
- DownloadDocument1 pageDownloadferrevNo ratings yet
- Trivedi. Post Laparascopic Treatment of Endometriosis With DYDDocument5 pagesTrivedi. Post Laparascopic Treatment of Endometriosis With DYDRuth RachmawatyNo ratings yet
- Comparative Study of Sublingual and Vaginal Misoprostol Tablet in Missed AbortionDocument7 pagesComparative Study of Sublingual and Vaginal Misoprostol Tablet in Missed AbortionIJAR JOURNALNo ratings yet
- 96FB0D241252Document4 pages96FB0D241252Adzana Yasadhy Hangga PrasetyoNo ratings yet
- Desmopressin Clinical PREADocument15 pagesDesmopressin Clinical PREAjoelrequenaNo ratings yet
- Gnrha Stop Protocol Versus Long Protocol in Poor Responder Ivf PatientsDocument6 pagesGnrha Stop Protocol Versus Long Protocol in Poor Responder Ivf PatientsGodha KiranaNo ratings yet
- 17Document7 pages17silvanaNo ratings yet
- 2012 Article 61Document5 pages2012 Article 61Al MubartaNo ratings yet
- Int J of Andrology - June 1994 - GEYTER - Peroxidase Positive Round Cells and Microorganisms in Human Semen Together WithDocument8 pagesInt J of Andrology - June 1994 - GEYTER - Peroxidase Positive Round Cells and Microorganisms in Human Semen Together WithmusaaabNo ratings yet
- JurnalDocument4 pagesJurnalAulia Rahma NoviastutiNo ratings yet
- Menyhei 1994Document4 pagesMenyhei 1994Anett Pappné LeppNo ratings yet
- Hospital Management: Bacterial InfectionDocument21 pagesHospital Management: Bacterial Infectionapadanainst7372No ratings yet
- Research ArticleDocument9 pagesResearch ArticleM RifkiNo ratings yet
- Asam TraneksamatDocument8 pagesAsam TraneksamatHamka KoersloNo ratings yet
- Dokazano Dejstvo Nigelle Sative (Crnog Kumina) U Eliminaciji Helicobacter PyloriDocument11 pagesDokazano Dejstvo Nigelle Sative (Crnog Kumina) U Eliminaciji Helicobacter PylorirbcollegeNo ratings yet
- 6 Relative Bio AvailabilityDocument4 pages6 Relative Bio AvailabilitymalagroudyNo ratings yet
- Dyq 030Document10 pagesDyq 030Marlintan Sukma AmbarwatiNo ratings yet
- Improved Survival Outcome of Childhood Acute Myeloid Leukemia With Intensified Chemotherapy in Chinese ChildrenDocument12 pagesImproved Survival Outcome of Childhood Acute Myeloid Leukemia With Intensified Chemotherapy in Chinese ChildrenneizhaNo ratings yet
- HTTP WWW - Sciencedirect.com Science Ob MImg& Imagekey B6WP1-4HK01J7-7-1& Cdi 6977& User 8187385& OrigDocument4 pagesHTTP WWW - Sciencedirect.com Science Ob MImg& Imagekey B6WP1-4HK01J7-7-1& Cdi 6977& User 8187385& OrigBimalKrishnaNo ratings yet
- Schiavi 2017Document8 pagesSchiavi 2017Naufal NanditaNo ratings yet
- A Systematic Review and Meta-Analysis of Ulipristal Acetate For Symptomatic Uterine FibroidsDocument8 pagesA Systematic Review and Meta-Analysis of Ulipristal Acetate For Symptomatic Uterine FibroidsHartanto LieNo ratings yet
- Appropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortDocument5 pagesAppropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortSiti Annisa NurfathiaNo ratings yet
- Teratogenic Effect of Carbamazepine Use During Pregnancy in The MiceDocument13 pagesTeratogenic Effect of Carbamazepine Use During Pregnancy in The MiceFeni YulindaNo ratings yet
- Agni Dagdha. Group-T Patients Were Treated With Indigenous Drugs and Group-C PatientsDocument14 pagesAgni Dagdha. Group-T Patients Were Treated With Indigenous Drugs and Group-C PatientsKrishnaNo ratings yet
- DTH 14650Document19 pagesDTH 14650Evelyn LimNo ratings yet
- WC 02 001Document1 pageWC 02 001Yuli HdyNo ratings yet
- tmp6EDE TMPDocument2 pagestmp6EDE TMPFrontiersNo ratings yet
- Lukaszuk Et Al. - 2005 - Optimization of Estradiol Supplementation During The Luteal Phase Improves The Pregnancy Rate in Women UnderDocument5 pagesLukaszuk Et Al. - 2005 - Optimization of Estradiol Supplementation During The Luteal Phase Improves The Pregnancy Rate in Women UnderKrzysztof ŁukaszukNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Grammar and PunctuationDocument11 pagesGrammar and Punctuationmohd_ikrayemNo ratings yet
- Science Grade 1Document3 pagesScience Grade 1mohd_ikrayemNo ratings yet
- Excel Sheets For Ivf CasesDocument2 pagesExcel Sheets For Ivf Casesmohd_ikrayemNo ratings yet
- Prime TechDocument32 pagesPrime Techmohd_ikrayemNo ratings yet
- Ago in The Past: DeterminerDocument9 pagesAgo in The Past: Determinermohd_ikrayemNo ratings yet
- Ultrasound Guidaed Embryo TransferDocument10 pagesUltrasound Guidaed Embryo Transfermohd_ikrayemNo ratings yet
- Using Excel To Graph A FunctionDocument2 pagesUsing Excel To Graph A Functionmohd_ikrayemNo ratings yet
- Siemens CU240E ReplacementDocument23 pagesSiemens CU240E ReplacementVăn Nghĩa NguyễnNo ratings yet
- CHUYÊN ĐỀ 19 - CÁC CẤP SO SÁNH - GRade B1,b2Document10 pagesCHUYÊN ĐỀ 19 - CÁC CẤP SO SÁNH - GRade B1,b2Thành Nam NguyễnNo ratings yet
- EX-CELL® EBx® PRO-II Serum-Free Medium Without L-Glutamine, Without Sodium BicarbonateDocument2 pagesEX-CELL® EBx® PRO-II Serum-Free Medium Without L-Glutamine, Without Sodium BicarbonateSAFC-GlobalNo ratings yet
- TOEFL Vocabulary 400 WordsDocument3 pagesTOEFL Vocabulary 400 WordsANGLISHT0% (1)
- Cbip Manual On RelayDocument2 pagesCbip Manual On RelayPrashant TrivediNo ratings yet
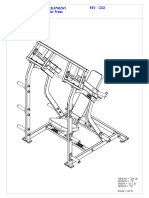
- HAMMER STRENGTH EQUIPMENT ILSP Iso Lateral Shoulder ...Document8 pagesHAMMER STRENGTH EQUIPMENT ILSP Iso Lateral Shoulder ...Rida DahmounNo ratings yet
- Wings of The SunDocument511 pagesWings of The Sunpatobotero043No ratings yet
- Tricks To Speed Up Calculations For Data Interpretation QuestionsDocument0 pagesTricks To Speed Up Calculations For Data Interpretation QuestionsR K MeenaNo ratings yet
- July & August Breakfast & Lunch MenuDocument2 pagesJuly & August Breakfast & Lunch Menujiwase2No ratings yet
- The Derivation Formula, Calculus Revision Notes From A-Level Maths TutorDocument4 pagesThe Derivation Formula, Calculus Revision Notes From A-Level Maths TutorA-level Maths TutorNo ratings yet
- DCL-01 Ex-01 NSDocument5 pagesDCL-01 Ex-01 NSankush2302No ratings yet
- The Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocument19 pagesThe Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PAAnonymous D29e00No ratings yet
- AGN142 - B Pole Slipping and Reverse PowerDocument3 pagesAGN142 - B Pole Slipping and Reverse PowerLaiqNo ratings yet
- Mysteries of The Convent of ChristDocument16 pagesMysteries of The Convent of ChristLuis Alfonso Bello RodríguezNo ratings yet
- SAT Problem Solving Practice Test 04Document3 pagesSAT Problem Solving Practice Test 04EszterListárNo ratings yet
- Liposomes 3Document63 pagesLiposomes 3Rohit SardaNo ratings yet
- The English Garden TourDocument318 pagesThe English Garden TourAlex_z4100% (4)
- ABB S200 Miniature Circuit BreakersDocument33 pagesABB S200 Miniature Circuit Breakersexge2000No ratings yet
- Aops Community 2010 Albania National OlympiadDocument1 pageAops Community 2010 Albania National OlympiadMuhammad Taufan FathurrachmanNo ratings yet
- T6N 800 PR221DS-LS/I in 800 4p F FDocument3 pagesT6N 800 PR221DS-LS/I in 800 4p F FOliver CelestialNo ratings yet
- Projectile MotionDocument29 pagesProjectile MotionLeague of Individuals for Environment SBCNo ratings yet
- Simulation of A Spin-Stabilised Sports Disc: W.J. Crowther and J.R. PottsDocument19 pagesSimulation of A Spin-Stabilised Sports Disc: W.J. Crowther and J.R. PottsdavpaffNo ratings yet
- Design With Nature: Ian Mcharg. The Natural History Press, New York, Ny, 1969. Review by Ashleigh GroseDocument1 pageDesign With Nature: Ian Mcharg. The Natural History Press, New York, Ny, 1969. Review by Ashleigh Groseanusha8204No ratings yet
- GATKwr12 3 IndelRealignment PDFDocument15 pagesGATKwr12 3 IndelRealignment PDFAlexander Louis SmithNo ratings yet
- Golden Gate Colleges P. Prieto ST., Batangas City: College of NursingDocument7 pagesGolden Gate Colleges P. Prieto ST., Batangas City: College of NursingR Hornilla ArcegaNo ratings yet
- VALERIAN Valeriana Officinalis HerbMedDocument31 pagesVALERIAN Valeriana Officinalis HerbMedNZHH100% (1)