You might also like
- Travel Insurance - Out of Province DetailsDocument2 pagesTravel Insurance - Out of Province DetailsMan DanaNo ratings yet
- How Much Should A Consultant CostDocument3 pagesHow Much Should A Consultant CostBogdanBNo ratings yet
- VRC-2301 (V10 Rate Card)Document2 pagesVRC-2301 (V10 Rate Card)lead sulphideNo ratings yet
- Output:: Item No. Unit Cost Annual Usage % Total Quantity Total Value % of Total Value Cum % of Total ValueDocument1 pageOutput:: Item No. Unit Cost Annual Usage % Total Quantity Total Value % of Total Value Cum % of Total ValueLeakhanakNguonNo ratings yet
- ExcelDocument2 pagesExcelapi-300241947No ratings yet
- Gold Extras Cover at a GlanceDocument3 pagesGold Extras Cover at a GlanceLaura Leander WildeNo ratings yet
- The Hopeful Family Team Final Project Fin 101 - Part BDocument22 pagesThe Hopeful Family Team Final Project Fin 101 - Part Bapi-314991266No ratings yet
- CONDICIONES DE FARODocument3 pagesCONDICIONES DE FARONorma VillegaNo ratings yet
- Barbados NemCare Individuals Health InsuranceDocument3 pagesBarbados NemCare Individuals Health InsuranceKammieNo ratings yet
- 44.pratibha Sahoo (Micro Economics)Document4 pages44.pratibha Sahoo (Micro Economics)SHREEMAYEE PANDANo ratings yet
- Binder 3-13141Document93 pagesBinder 3-13141Anubhav JainNo ratings yet
- AISAUCES2Document8 pagesAISAUCES2jlehartNo ratings yet
- Multiple RegressionDocument4 pagesMultiple Regressionsumit kumarNo ratings yet
- 2015 Brackets & Planning Limits (Janney)Document5 pages2015 Brackets & Planning Limits (Janney)John CortapassoNo ratings yet
- Kitov China DealDocument1 pageKitov China DealAnonymous ipErpL6No ratings yet
- StickkDocument4 pagesStickkNikesh PatelNo ratings yet
- Brochure PDF MANHATTHAN LIFEDocument2 pagesBrochure PDF MANHATTHAN LIFEEmanuel ChirinosNo ratings yet
- Daily Profit CalculatorDocument9 pagesDaily Profit CalculatorHarrati IliasNo ratings yet
- Maru Betting Center Excel SheetDocument16 pagesMaru Betting Center Excel SheetRohan ShahNo ratings yet
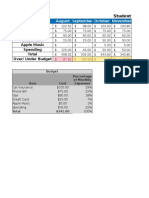
- Budget Variance ReportDocument2 pagesBudget Variance ReportaryanneNo ratings yet
- Analisis Suturas 2020Document6 pagesAnalisis Suturas 2020David SantoandreNo ratings yet
- Premium Table Plus Rider EISDocument2 pagesPremium Table Plus Rider EISHarry SmithNo ratings yet
- Libro 1Document2 pagesLibro 1yonathanNo ratings yet
- Libro 1Document2 pagesLibro 1yonathanNo ratings yet
- BudgetDocument2 pagesBudgetMitch FelsmanNo ratings yet
- OAN AND Avings Ates: Loan Rates - Effective As of July 24, 2013Document1 pageOAN AND Avings Ates: Loan Rates - Effective As of July 24, 2013indianbuddyNo ratings yet
- Your Customized Benefits Plan at HCL America IncDocument2 pagesYour Customized Benefits Plan at HCL America IncShiv RanjanNo ratings yet
- Premium Table Deluxe Rider EISDocument2 pagesPremium Table Deluxe Rider EISHarry SmithNo ratings yet
- Cuadro de MarchaDocument1 pageCuadro de MarchaJoaco LledxNo ratings yet
- Mec 31 Act05Document1 pageMec 31 Act05chinNo ratings yet
- Fin 3060 IncomestatementDocument2 pagesFin 3060 Incomestatementapi-295008203No ratings yet
- Analysis of investment alternatives using IRRDocument7 pagesAnalysis of investment alternatives using IRRmeta pratiwiNo ratings yet
- Tithe - Percentage Giving ChartDocument1 pageTithe - Percentage Giving ChartRay Anthony Rodriguez0% (1)
- Excell FinalDocument1 pageExcell Finalapi-248089671No ratings yet
- Indic AdoresDocument139 pagesIndic AdoresAndreyPonteNo ratings yet
- Workbook 2Document3 pagesWorkbook 2api-332346855No ratings yet
- Resturant Break Even Analysis v4Document4 pagesResturant Break Even Analysis v4chris51bNo ratings yet
- Premier 3-28-14Document1 pagePremier 3-28-14api-239720148No ratings yet
- New Hire Benefits Summary: Medical, PTO, Life Ins & MoreDocument3 pagesNew Hire Benefits Summary: Medical, PTO, Life Ins & MoreRavi Prakash MayreddyNo ratings yet
- Stud-E PresentationDocument13 pagesStud-E Presentationapi-242374745No ratings yet
- Estimate weekly bike rental demand using linear regressionDocument6 pagesEstimate weekly bike rental demand using linear regressionMrunmaiNo ratings yet
- Numero Referencia Valor Total % Costo Unitario Unidades Demanda Anual Porcentaje AcumuladoDocument3 pagesNumero Referencia Valor Total % Costo Unitario Unidades Demanda Anual Porcentaje Acumuladoyenni viloriaNo ratings yet
- Revenue ForecastDocument3 pagesRevenue ForecastMarc BeaupréNo ratings yet
- Vista NB Special Offer February 2020Document2 pagesVista NB Special Offer February 2020aneeshNo ratings yet
- Excel Chapter 2 - Lab Test ADocument2 pagesExcel Chapter 2 - Lab Test AFurqan Ali KhanNo ratings yet
- Traffic intersection improvement cost analysisDocument1 pageTraffic intersection improvement cost analysisUn Tal Alberto MelendezNo ratings yet
- Forex Trading Income CalculatorDocument14 pagesForex Trading Income CalculatorPrashantPatilNo ratings yet
- Sample Development CostsDocument1 pageSample Development Costsrahul240486No ratings yet
- Key Financial Indicators For Spa SuccessDocument34 pagesKey Financial Indicators For Spa SuccessdclmanNo ratings yet
- Why Rent When You Can Buy?: Buying Costs Less Per Month. Down Payment Can Be A GiftDocument1 pageWhy Rent When You Can Buy?: Buying Costs Less Per Month. Down Payment Can Be A Giftapi-328599640No ratings yet
- All Dollar Values in Millions: Operating InformationDocument15 pagesAll Dollar Values in Millions: Operating InformationJose Hines-AlvaradoNo ratings yet
- TABL2751 Tax Rates 2021 - UpdatedDocument4 pagesTABL2751 Tax Rates 2021 - UpdatedPeper12345No ratings yet
- EQ Employee Benefits Plan Brochure (January 2023)Document8 pagesEQ Employee Benefits Plan Brochure (January 2023)Darren ChenNo ratings yet
- NSTP 1Document4 pagesNSTP 1MelbaNo ratings yet
- Total RevenueDocument1 pageTotal RevenueethanselphNo ratings yet
- Marks of Gyne-2 For 6Th Year Medical Students 2016/2017Document4 pagesMarks of Gyne-2 For 6Th Year Medical Students 2016/2017Bariqah SalahNo ratings yet
- Dental Practice BSC ReportDocument46 pagesDental Practice BSC ReportlnhpNo ratings yet
- Stock Trading P&L AnalysisDocument5 pagesStock Trading P&L AnalysisSilat KaliNo ratings yet