You might also like
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocument13 pagesOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- John Deere Troubleshooting - 31200371Document64 pagesJohn Deere Troubleshooting - 31200371Tesla Ec100% (7)
- Chemsheets As 1092 IR SpectrosDocument4 pagesChemsheets As 1092 IR Spectroscharlesma123No ratings yet
- Arterial Blood Gas Analysis PDFDocument2 pagesArterial Blood Gas Analysis PDFJim Jose Antony100% (3)
- Procedure Checklist Chapter 19: Assessing The Chest and LungsDocument2 pagesProcedure Checklist Chapter 19: Assessing The Chest and LungsjthsNo ratings yet
- Ethical Issues in AnaesthesiaDocument23 pagesEthical Issues in AnaesthesiaEverton McIntosh0% (1)
- Cell PhysiologyDocument61 pagesCell Physiologykiedd_04100% (4)
- Heart SoundDocument15 pagesHeart SoundLilian EdeniNo ratings yet
- Lung SoundsDocument24 pagesLung SoundsAswinNo ratings yet
- Vital Sign:Pulse: Prepared By: Mrs Bemina Ja Assistant Professor ESIC College of Nursing KalaburagiDocument38 pagesVital Sign:Pulse: Prepared By: Mrs Bemina Ja Assistant Professor ESIC College of Nursing Kalaburagibemina jaNo ratings yet
- SHOCKDocument35 pagesSHOCKsami azadNo ratings yet
- Anatomy & Physiology of The Cardiovascular SystemDocument3 pagesAnatomy & Physiology of The Cardiovascular SystemluaNo ratings yet
- Mitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeDocument16 pagesMitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeAsrafur RahmanNo ratings yet
- Lung Biopsy 1Document1 pageLung Biopsy 1Sivaprasad SNo ratings yet
- NebulizationDocument4 pagesNebulizationleoNo ratings yet
- Lung AuscultationDocument62 pagesLung AuscultationOlea CroitorNo ratings yet
- Pneumonia: DefinitionDocument5 pagesPneumonia: DefinitionhemaanandhyNo ratings yet
- Synthetic Antibacterial AgentsDocument58 pagesSynthetic Antibacterial AgentsApurba Sarker Apu100% (3)
- Administration of Inotropes Evidence Based Nursing PolicyDocument8 pagesAdministration of Inotropes Evidence Based Nursing PolicyRonald ThakorNo ratings yet
- Anatomy and Physiology of Hearing SystemDocument63 pagesAnatomy and Physiology of Hearing SystemKharenza Vania Azarine Bachtiar100% (1)
- Cardiac AssessmentDocument48 pagesCardiac AssessmentRatheesh NathNo ratings yet
- ANGIOGRAPHYDocument8 pagesANGIOGRAPHYAkazukin AineNo ratings yet
- Tracheostomy Set ContainingDocument10 pagesTracheostomy Set ContainingShivani DhillonNo ratings yet
- Breathing and Incentive SpirometryDocument41 pagesBreathing and Incentive SpirometryVillain DevilNo ratings yet
- Ca LarynxDocument36 pagesCa LarynxTito PNo ratings yet
- CT KubDocument2 pagesCT KubKumail KhandwalaNo ratings yet
- 1st Chap-2Document40 pages1st Chap-2RJ Noor JanNo ratings yet
- Doppler Ultrasound - L1Document24 pagesDoppler Ultrasound - L1quickdannyNo ratings yet
- Tracheobronchial TreeDocument51 pagesTracheobronchial TreeravishNo ratings yet
- CVADocument13 pagesCVAAmlan jyoti thanapatiNo ratings yet
- ... 2 Finals Pulmonary PhysiologyDocument9 pages... 2 Finals Pulmonary PhysiologyELIZABETH GRACE AMADOR100% (1)
- Cardiovascular System Lab 2007Document12 pagesCardiovascular System Lab 2007Nikita JacobsNo ratings yet
- Syncope: - Selvarathi KDocument27 pagesSyncope: - Selvarathi KSelvarathi KandhaswamyNo ratings yet
- 7.shashank M - Physical and Chemical Agents-1Document28 pages7.shashank M - Physical and Chemical Agents-1Manojna KMNo ratings yet
- Cardiovascular System: by DR - Nuha Abdel GhaffarDocument41 pagesCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanNo ratings yet
- Chest and LungsDocument49 pagesChest and LungsChala KeneNo ratings yet
- Advanced Cardiac ProcedureDocument9 pagesAdvanced Cardiac ProcedureSachin DwivediNo ratings yet
- PY 5.16: Record Arterial Pulse Tracing Using Finger Plethysmography in A Volunteer or Simulated EnvironmentDocument6 pagesPY 5.16: Record Arterial Pulse Tracing Using Finger Plethysmography in A Volunteer or Simulated EnvironmentADITYA SARAFNo ratings yet
- Broncho Pulmonary SegmentsDocument2 pagesBroncho Pulmonary SegmentsSyeda SapnaNo ratings yet
- Eye ExaminationDocument23 pagesEye Examinationcynthia167No ratings yet
- Purbanchal University Shree Medical and Technical College Bharatpur 10, ChitwanDocument10 pagesPurbanchal University Shree Medical and Technical College Bharatpur 10, Chitwansushma shresthaNo ratings yet
- Respiratory System - Anatomy & PhysiologyDocument24 pagesRespiratory System - Anatomy & PhysiologySarthak ShahNo ratings yet
- ThoracentesisDocument4 pagesThoracentesisCyntia Theresia Lumintang100% (1)
- Head Injury OkeDocument42 pagesHead Injury OkeAnonymous p9msXAEwNo ratings yet
- Seizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HDocument70 pagesSeizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HRohini RaiNo ratings yet
- Chemo ReceptorDocument8 pagesChemo ReceptorCheryl Lyn SanchezNo ratings yet
- Barium Swallow: DR Akash Bhosale Jr1Document66 pagesBarium Swallow: DR Akash Bhosale Jr1Aakash BhosaleNo ratings yet
- Empyema 171013100219Document23 pagesEmpyema 171013100219Mahmoud Abdel MoneimNo ratings yet
- Wound Dressing Procedure WPS OfficeDocument8 pagesWound Dressing Procedure WPS OfficeAbhishek VermaNo ratings yet
- PacemakerDocument13 pagesPacemakeralainzkie100% (2)
- Holter MonitoringDocument21 pagesHolter MonitoringAngel LeeNo ratings yet
- Cerebrovascular AccidentDocument30 pagesCerebrovascular AccidentJaydee Dalay100% (2)
- Approach To An Unconscious Patient-OyeyemiDocument41 pagesApproach To An Unconscious Patient-OyeyemiOyeyemi AdeyanjuNo ratings yet
- LUNG-OVERVIEW (Autosaved)Document132 pagesLUNG-OVERVIEW (Autosaved)Thivashinie Kandy Nazan VelloNo ratings yet
- Heart Sounds: They Are The Sounds Produced by The Mechanical Activities of The Heart During Each Cadiac CycleDocument19 pagesHeart Sounds: They Are The Sounds Produced by The Mechanical Activities of The Heart During Each Cadiac Cyclevishnudurga100% (1)
- Thoracic Inlet Syndrome and Cervical RibDocument28 pagesThoracic Inlet Syndrome and Cervical RibRabin DasNo ratings yet
- Holter MonitoringDocument19 pagesHolter Monitoringomotola Ayobundle-oyewo MA206100% (1)
- Leprosy PDFDocument19 pagesLeprosy PDFsteffiecruz06No ratings yet
- Thoracotomy: Surgery For Lung ProblemsDocument14 pagesThoracotomy: Surgery For Lung ProblemsPutri ChalqieNo ratings yet
- Airway Obstruction Final2Document33 pagesAirway Obstruction Final2Mahindra KumarNo ratings yet
- UnconsciousnessDocument16 pagesUnconsciousnessAkhilesh BabuNo ratings yet
- LungsDocument5 pagesLungsabbaslafe0% (1)
- Hemodynamic MonitoringDocument4 pagesHemodynamic Monitoringgurneet kourNo ratings yet
- L6) Heart SoundsDocument30 pagesL6) Heart SoundsMar Lar LwinNo ratings yet
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Document2 pagesIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04No ratings yet
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- "Traditional" Exegeses of Q 4:34Document15 pages"Traditional" Exegeses of Q 4:34kiedd_04No ratings yet
- SYNAPSEDocument35 pagesSYNAPSEkiedd_04100% (3)
- The Place For Others in IslamDocument27 pagesThe Place For Others in Islamkiedd_04No ratings yet
- Fadhilat Surah at TakwirDocument1 pageFadhilat Surah at Takwirkiedd_04No ratings yet
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- Microbiology Colour Plate No.7Document1 pageMicrobiology Colour Plate No.7kiedd_04No ratings yet
- Microbiology Colour Plate No.9Document1 pageMicrobiology Colour Plate No.9kiedd_04No ratings yet
- Microbiology Colour Plate No.4Document1 pageMicrobiology Colour Plate No.4kiedd_04No ratings yet
- Microbiology Colour Plate No.5Document1 pageMicrobiology Colour Plate No.5kiedd_04No ratings yet
- API® CoryneDocument4 pagesAPI® Corynekiedd_04No ratings yet
- Microbiology Colour Plate No.6Document1 pageMicrobiology Colour Plate No.6kiedd_04No ratings yet
- Microbiology Colour Plate No.8Document1 pageMicrobiology Colour Plate No.8kiedd_04No ratings yet
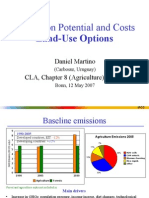
- Mitigation Potential and Costs Land-Use OptionsDocument9 pagesMitigation Potential and Costs Land-Use Optionskiedd_04No ratings yet
- Microbiology Colour Plate No.1Document1 pageMicrobiology Colour Plate No.1kiedd_04No ratings yet
- Microbiology Colour Plate No.3Document1 pageMicrobiology Colour Plate No.3kiedd_04No ratings yet
- Carnitine DeficiencyDocument21 pagesCarnitine Deficiencykiedd_04100% (1)
- Mitigation of Climate ChangeDocument41 pagesMitigation of Climate Changekiedd_04No ratings yet
- Microbiology Colour Plate No.2Document1 pageMicrobiology Colour Plate No.2kiedd_04No ratings yet
- Mitigation of Climate ChangeDocument25 pagesMitigation of Climate Changekiedd_04No ratings yet
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocument10 pagesPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04No ratings yet
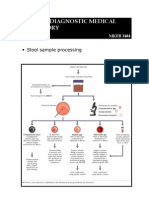
- Stool Sample ProcessingDocument1 pageStool Sample Processingkiedd_04No ratings yet
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocument1 pageAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
- Diagram of Classification of EnterobacteriaDocument1 pageDiagram of Classification of Enterobacteriakiedd_04100% (1)
- Oxidase TestDocument1 pageOxidase Testkiedd_04100% (1)
- Mothers and Adolescent Sons: The Unique Role of A Mother in The Life of Her Adolescent SonDocument26 pagesMothers and Adolescent Sons: The Unique Role of A Mother in The Life of Her Adolescent SonTauseef AhmadNo ratings yet
- STLE2018 - Grease I - Session 3I - E. Casserly - The Effect of Base Oils On Thickening and Physical PropertiesDocument2 pagesSTLE2018 - Grease I - Session 3I - E. Casserly - The Effect of Base Oils On Thickening and Physical PropertiesCharles RichardNo ratings yet
- Hydrochloric Acid, 0.1N (0.1M) : Safety Data SheetDocument7 pagesHydrochloric Acid, 0.1N (0.1M) : Safety Data SheetRandu AgungS1 Teknik kimiaNo ratings yet
- Bell Coleman CycleDocument5 pagesBell Coleman CycleAshara Aakash100% (2)
- ENSO ReportDocument18 pagesENSO ReportMALABIKA MONDALNo ratings yet
- Agrofood Sistema Vrie 2012Document40 pagesAgrofood Sistema Vrie 2012PaulinaNo ratings yet
- She 9.5 TravellerDocument11 pagesShe 9.5 TravellerBen WooffNo ratings yet
- Speech ContestDocument1 pageSpeech ContestLutfan LaNo ratings yet
- Specifications Eh 500fDocument7 pagesSpecifications Eh 500fElfirman Syafei100% (1)
- Iss 3 KM280 Multilingual PDFDocument162 pagesIss 3 KM280 Multilingual PDFCristina AndreiNo ratings yet
- Reguli Certificare NFDocument194 pagesReguli Certificare NFAndriciuc Ionut100% (1)
- Animal Slaughterhouse and Meat Inspection Act 2055: DR.R.P Yadav M.SC (Meat Tech)Document26 pagesAnimal Slaughterhouse and Meat Inspection Act 2055: DR.R.P Yadav M.SC (Meat Tech)Dhiraj BoharaNo ratings yet
- 1606 Organic World 2013Document340 pages1606 Organic World 2013Marius VrajaNo ratings yet
- Formulation and Evaluation of Amlodipine Fast Dissolving TabletsDocument9 pagesFormulation and Evaluation of Amlodipine Fast Dissolving TabletsEditor IJTSRDNo ratings yet
- Respiratory SystemDocument89 pagesRespiratory SystemMuhammad HanifNo ratings yet
- Ufc 4 510 0 PDFDocument419 pagesUfc 4 510 0 PDFsajuhereNo ratings yet
- P0883-Tcm Power Input High: For A Complete Wiring Diagram, Refer To The Wiring InformationDocument6 pagesP0883-Tcm Power Input High: For A Complete Wiring Diagram, Refer To The Wiring InformationElias RondónNo ratings yet
- Sex, Status, and Social Reproduction PDFDocument45 pagesSex, Status, and Social Reproduction PDFT.No ratings yet
- Duties of A Scrub NurseDocument43 pagesDuties of A Scrub Nursejay kusainNo ratings yet
- Coca-Cola As A Global Brand in Relation To Perception and Preference of Consumers in Karachi Part IIDocument93 pagesCoca-Cola As A Global Brand in Relation To Perception and Preference of Consumers in Karachi Part IIstephan006100% (1)
- Beyond Strange - True Tales of A - Rob MacGregorDocument137 pagesBeyond Strange - True Tales of A - Rob MacGregorKimo120% (1)
- Protein 3dDocument86 pagesProtein 3dSitiHamidatulAliyahNo ratings yet
- Methylamine RecipeDocument4 pagesMethylamine RecipeVanilla470% (1)
- Shashirekha H K PDFDocument222 pagesShashirekha H K PDFpk50% (2)
- Gender Differences in Classroom Participation: The Case of Second and Third Secondary Year Foreign Languages Classes - JijelDocument152 pagesGender Differences in Classroom Participation: The Case of Second and Third Secondary Year Foreign Languages Classes - JijelelKaicer100% (2)
- Sustainable AgricultureDocument8 pagesSustainable AgricultureMd. AssaduzzamanNo ratings yet
- MMS Appraisal and Development of Pipeline Defect Assessment MethodsDocument172 pagesMMS Appraisal and Development of Pipeline Defect Assessment MethodsEyoma EtimNo ratings yet