Nursing Care Plan
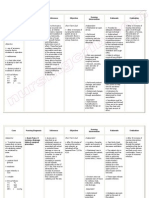
Ineffective airway clearance
Cues Nursing Planning Intervention Rationale Evaluation
Diagnosis
I- “nahihirapan Ineffective After nursing To maintain Goes met the
ako huminga airway intervention the adequate patient client able to
at kapag clearance patient will able to airway the nurse maintain
umuubo ako related to Objectives: manage will able: airway
may asthma as a and maintain a. monitor Indicative of clearance and
kasamang manifested by airway patency. respiration respiratory clear
plema” as difficulty of After 2hrs. nursing & breath distress or secretions
verbalized by breathing. intervention the sound, accumulation readily.
the patient. patient will: noting rate of secretion.
a. Verbalize & sounds
O- Difficulty & understandin (e.g.
rapidly in g of causes & tachypnea,
breathing. therapeutic crackles,
management wheezes.)
M- RR-23 bpm regimen b. Elevate
BP-100/70 within head of To take
PR-82 bpm 20mins. bed/change advantage of
T- 37.3 b. Demonstrate position gravity
behavior to every 2hrs. decreasing,
improve & prn. pressure on
maintain the diaphragm
clear airway & enhancing
within c. Keep drainage of
30mins. environment ventilation to
c. Demonstrate allergen free diff. lung
reduction of (e.g.broncho segment.
congestion w/ scopy
breath tracheotomy To clear/
sounds clear ) maintain open
respiration d. To mobilize airway.
noiseless secretion
improved encourage
oxygen deep
exchange breathing &
within coughing
30mins. exercise
d. Identify splint
potential chest/incisio To maximize
complication n. effort.
on how to Dependent;
initiate administer
appropriate analgesic
preventive or Give
corrective expectorant
actions within s or
20mins. bronchodilat
ors as To improve
ordered. cough when
To promote pain is
wellness; inhibiting
demonstrate effort.
client in
performing
specific
airway
clearance
technique.
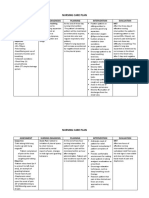
Cues Nursing Planning or Nursing Rationale Evaluation
Diagnosis Goal Intervention
I: “My incision •Acute pain •After 2 hrs nursing •Use pain rating •To evaluate •Goals
site is so related to intervention the scale appropriate patient partially met.
painful” as physical patient will: for age/cognition response to The patient
verbalize by factor e.g., pain. able to control
the patient. disruption of •Decrease pain •Observe and reduce
skin & tissue rate from 5 to 2 nonverbal pain.
O: Presence of (incision) as cues/pain •Observations
facial grimace evidence by •Report pain is behaviors. may/may not •From pain
when reports of relieved/controlled. be congruent rate of 5
palpation the pain and with verbal decrease to 3.
abdominal guarding at reports or may
area and the area. be only
guarding the indicator
area when present when
assessing it. •Encourage patient is
adequate rest unable to
M: periods. verbalize.
•BP- 100/70
mmhg •To prevent
•T- 37.3°C fatigue.
•PR- 89 bpm
•RR- 19
•Pain scale-
5/10
You might also like
- NCP Ineffective Airway ClearanceDocument5 pagesNCP Ineffective Airway ClearanceEmm Estipona HaoNo ratings yet
- NCP Ineffective Airway ClearanceDocument4 pagesNCP Ineffective Airway ClearanceMary Joyce Limoico100% (1)
- Ineffective Airway ClearanceDocument1 pageIneffective Airway Clearancerozj0750% (2)
- Ineffective Airway Clearance Related To BronchospasmDocument2 pagesIneffective Airway Clearance Related To BronchospasmReylan Garcia100% (4)
- Impaired Gas Exchange-Sample NCPDocument1 pageImpaired Gas Exchange-Sample NCPKaycee BinanNo ratings yet
- Asthma Impaired Gas ExchangeDocument2 pagesAsthma Impaired Gas ExchangeNedeve Ozned100% (5)
- Pneumonia-Ineffective Airway ClearanceDocument2 pagesPneumonia-Ineffective Airway ClearanceNursesLabs.com86% (7)
- Nursing Care Plan Ineffective Airway Clearance (Bronchi)Document2 pagesNursing Care Plan Ineffective Airway Clearance (Bronchi)deric94% (17)
- Nursing Care Plan Ineffective Airway ClearanceDocument3 pagesNursing Care Plan Ineffective Airway Clearancederic100% (13)
- NCP Ineffective Airway Clearance Related To Excessive Mucus Production COPDDocument7 pagesNCP Ineffective Airway Clearance Related To Excessive Mucus Production COPDMa. Elaine Carla Tating67% (3)
- NCP Ineffective Airway Clearance Related To The Accumulation of Exudates in The Alveoli TBDocument3 pagesNCP Ineffective Airway Clearance Related To The Accumulation of Exudates in The Alveoli TBMa. Elaine Carla Tating0% (1)
- NURSING-CARE-PLAN-Lung-Cancerxxx 1Document3 pagesNURSING-CARE-PLAN-Lung-Cancerxxx 1Caroline ChaNo ratings yet
- NCP - CapDocument4 pagesNCP - CapSherryNo ratings yet
- NCP - Ineffective Airway ClearanceDocument2 pagesNCP - Ineffective Airway Clearancelarapatricia1215No ratings yet
- Activity IntoleranceDocument3 pagesActivity IntoleranceGen RodriguezNo ratings yet
- Acute Pain Related To Inflammation of Tissues Secondary To AppendicitisDocument2 pagesAcute Pain Related To Inflammation of Tissues Secondary To AppendicitisRachel SaavedraNo ratings yet
- Assessing and Managing Respiratory DistressDocument3 pagesAssessing and Managing Respiratory DistressGen RodriguezNo ratings yet
- NCP Ineffective Airway Clearance Related To The Accumulation of Secretions As Evidence by Decrease in Respiratory Rate and NGT and ET Tube Attached and Crackles at The Left Base of The LungsDocument3 pagesNCP Ineffective Airway Clearance Related To The Accumulation of Secretions As Evidence by Decrease in Respiratory Rate and NGT and ET Tube Attached and Crackles at The Left Base of The LungsSarah Ann Jamilla FaciolanNo ratings yet
- NCP Impaired Gas ExchangeDocument2 pagesNCP Impaired Gas ExchangeCharissa Magistrado De LeonNo ratings yet
- Nursing Care Plan For Ineffective Airway ClearanceDocument7 pagesNursing Care Plan For Ineffective Airway Clearancearlee marquez96% (117)
- NCP Ineffective Breathing Pattern TalaDocument1 pageNCP Ineffective Breathing Pattern TalaJhen Bitco Fidel70% (10)
- Nursing Care Plan Assessment Diagnosis Planning Implementation Rationale EvaluationDocument1 pageNursing Care Plan Assessment Diagnosis Planning Implementation Rationale EvaluationMyrien BanaagNo ratings yet
- Ineffective Breathing PatternDocument1 pageIneffective Breathing Patternimneverwrong249280% (5)
- Ineffective Breathing PatternDocument5 pagesIneffective Breathing PatternruguNo ratings yet
- NCP For Ineffective Airway Clearance.Document2 pagesNCP For Ineffective Airway Clearance.Vanessa Joy Contreras100% (1)
- Ineffective Breathing Pattern Pneumonia Nursing Care PlanDocument1 pageIneffective Breathing Pattern Pneumonia Nursing Care PlanJasonlee BaluyotNo ratings yet
- Final NCP Ineffective Airway ClearanceDocument8 pagesFinal NCP Ineffective Airway ClearanceHazel EndayaNo ratings yet
- Assessing Impaired Gas ExchangeDocument1 pageAssessing Impaired Gas ExchangeRryje Salleva100% (1)
- Nursing Care Plan: Subjective: Short Term IndependentDocument2 pagesNursing Care Plan: Subjective: Short Term IndependentKristine Young50% (2)
- Impaired Gas Exchange NCPDocument4 pagesImpaired Gas Exchange NCPkimglaidyl bontuyanNo ratings yet
- NCP Ineffective Airway ClearanceDocument2 pagesNCP Ineffective Airway Clearanceniomi0884% (31)
- NCP For AsthmaDocument1 pageNCP For AsthmaMelvin Martinez100% (1)
- Nursing Care Plan - Ineffective Airway ClearanceDocument1 pageNursing Care Plan - Ineffective Airway ClearanceLei OrtegaNo ratings yet
- NCP Ineffective Airway Clearance For PneumoniaDocument5 pagesNCP Ineffective Airway Clearance For PneumoniaKullin Rain100% (1)
- NCP For FeverDocument2 pagesNCP For FeverDominises Jade Corpuz82% (17)
- Ineffective Airway Clearance Related To Retained Mucus Secretion As Evidenced by Unproductive CoughDocument1 pageIneffective Airway Clearance Related To Retained Mucus Secretion As Evidenced by Unproductive Coughdana93% (30)
- Nursing Measures To Maintain Normal Respiratory Function and OxygenationDocument2 pagesNursing Measures To Maintain Normal Respiratory Function and Oxygenationlodeth100% (2)
- NCPDocument4 pagesNCPEsther RefuncionNo ratings yet
- Vii. Nursing Care Plan: Nursing Diagnosis Prioritization SignificanceDocument7 pagesVii. Nursing Care Plan: Nursing Diagnosis Prioritization SignificanceMarichu Bajado0% (1)
- Student NurseDocument2 pagesStudent NurseTAYABAN, KENNETH JAKE, Q.No ratings yet
- Acute Pancreatitis Assessment Diagnosis Planning Intervention EvaluationDocument6 pagesAcute Pancreatitis Assessment Diagnosis Planning Intervention EvaluationmichelsorianoNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaNo ratings yet
- Problem: Viii. Planning (Nursing Cre Plan)Document10 pagesProblem: Viii. Planning (Nursing Cre Plan)Raidis PangilinanNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Planning Intervention EvaluationDocument4 pagesNursing Care Plan: Assessment Nursing Diagnosis Planning Intervention EvaluationGiddel Guerra PapellerasNo ratings yet
- Vii. Nursing Care Plan Assessment Nursing Diagnosis Plan of Care Expected Outcome Evaluation Subjective: Independent: Short Term GoalDocument1 pageVii. Nursing Care Plan Assessment Nursing Diagnosis Plan of Care Expected Outcome Evaluation Subjective: Independent: Short Term Goalapi-3828211No ratings yet
- CuesDocument2 pagesCuesAndrea Love PalomoNo ratings yet
- Asthma NCPDocument3 pagesAsthma NCPjaijai magbanuaNo ratings yet
- NCP SciDocument3 pagesNCP SciJaylord VerazonNo ratings yet
- Vi. Nursing Care PlanDocument3 pagesVi. Nursing Care PlanJopaii TanakaNo ratings yet
- Assessment Nursing Diagnosis Plan of Care Expected Outcome Evaluation Subjective: Independent: Short Term Goal: Goals MetDocument2 pagesAssessment Nursing Diagnosis Plan of Care Expected Outcome Evaluation Subjective: Independent: Short Term Goal: Goals Metapi-3828211No ratings yet
- Ix. Nursing Care PlanDocument6 pagesIx. Nursing Care PlanJai - HoNo ratings yet
- Assessment, Diagnosis, Planning, Intervention and Evaluation of a Client with Increased Airway SecretionsDocument3 pagesAssessment, Diagnosis, Planning, Intervention and Evaluation of a Client with Increased Airway SecretionsNicholas TagleNo ratings yet
- Cues Nursing Diagnos Is Backgro Und Knowled Ge Goals and Objectives Nursing Intervention and Rationale EvaluationDocument3 pagesCues Nursing Diagnos Is Backgro Und Knowled Ge Goals and Objectives Nursing Intervention and Rationale EvaluationSkyla FiestaNo ratings yet
- Valeriano, NCPDocument4 pagesValeriano, NCPVALERIANO TRISHANo ratings yet
- Nursing Care Plan Bronchial AsthmaDocument2 pagesNursing Care Plan Bronchial Asthmaderic93% (60)
- FAELDONEA, PJ - Nursing Care PlanDocument6 pagesFAELDONEA, PJ - Nursing Care PlanPatricia Jean Faeldonea100% (1)
- NCP Copd FinalDocument3 pagesNCP Copd FinalGiselle EstoquiaNo ratings yet
- Difficulty Breathing Nursing Care PlanDocument3 pagesDifficulty Breathing Nursing Care PlanOPERAñA ELLAYZA RB DECANONo ratings yet
- Nursing Care Plan: Assessm ENT Nursing Diagnos IS Planning Intervention Rationale Evaluati ON Subjectiv eDocument4 pagesNursing Care Plan: Assessm ENT Nursing Diagnos IS Planning Intervention Rationale Evaluati ON Subjectiv eJ. TSNo ratings yet
- Asthma Attack Nursing Care Plan for Married Female PatientDocument5 pagesAsthma Attack Nursing Care Plan for Married Female PatientMarivic Yuson MalagarNo ratings yet
- Group 1 Case Study Chapter 24Document10 pagesGroup 1 Case Study Chapter 24Doneva Lyn MedinaNo ratings yet
- Evaluasi Penggunaan Obat Pada Pasien Ppok (Penyakit ParuDocument9 pagesEvaluasi Penggunaan Obat Pada Pasien Ppok (Penyakit ParuApriyatunNo ratings yet
- Drug Study on Salbutamol for Pediatric NursingDocument9 pagesDrug Study on Salbutamol for Pediatric NursingCrizza JoyceNo ratings yet
- Case Study-ASTHMADocument19 pagesCase Study-ASTHMAFritzielove BayawaNo ratings yet
- Examination of The Respiratory SystemDocument35 pagesExamination of The Respiratory SystemRashhmi Karthodi100% (1)
- BerodualDocument1 pageBerodualAelysa PabloNo ratings yet
- BulSU-CON Nursing Health Teaching Plan on Asthma RisksDocument5 pagesBulSU-CON Nursing Health Teaching Plan on Asthma RisksKervin Jude D. ManahanNo ratings yet
- Asthma in PregnancyDocument9 pagesAsthma in PregnancyMaria Claudia Pevez LoveraNo ratings yet
- Soap Notes AsthmaDocument6 pagesSoap Notes AsthmaCHRISTINE KARENDINo ratings yet
- v13n3 CPG UpdateDocument7 pagesv13n3 CPG UpdateedfZSEADFsfsafafNo ratings yet
- CH 25 Respiration Study GuideDocument2 pagesCH 25 Respiration Study Guide99646qbkdwNo ratings yet
- Acid Base Activity ANSWERSDocument1 pageAcid Base Activity ANSWERSTuTitNo ratings yet
- Inhalation Injury and Systemic IntoxicationDocument7 pagesInhalation Injury and Systemic IntoxicationDaniel LesmanaNo ratings yet
- Idoc - Pub Ncp-SinusitisDocument2 pagesIdoc - Pub Ncp-SinusitisEdson John Demayo100% (1)
- Invitation Webinar Asma PDPI 17sep2023Document2 pagesInvitation Webinar Asma PDPI 17sep2023Muhammad Agil Wijaya FaradisNo ratings yet
- Breathing Pattern DiagnosisDocument2 pagesBreathing Pattern DiagnosisLyca Mae AurelioNo ratings yet
- Lab 06 SpirometryDocument28 pagesLab 06 SpirometryMâřâh MöHămmădNo ratings yet
- Ipratroprium Drug CardDocument3 pagesIpratroprium Drug CardXiaoDuckyNo ratings yet
- NCP AsthmaDocument5 pagesNCP AsthmaJu Lie AnnNo ratings yet
- Activity 1.1 Journey of A Breath of AirDocument4 pagesActivity 1.1 Journey of A Breath of AirJorjette Kate BatuNo ratings yet
- Hyperoxia: Jed Wolpaw, MD, M.EdDocument71 pagesHyperoxia: Jed Wolpaw, MD, M.EdJustin WangNo ratings yet
- Ian Govias Gaynor Mitchell - Asthma Education Principles and Practice For The Asthma Educator.-Springer Nature (2021)Document660 pagesIan Govias Gaynor Mitchell - Asthma Education Principles and Practice For The Asthma Educator.-Springer Nature (2021)Алина КостюковаNo ratings yet
- MSU-Iligan Institute of Technology College of Nursing: Level II AACUP AccreditedDocument4 pagesMSU-Iligan Institute of Technology College of Nursing: Level II AACUP AccreditedChristine Pialan SalimbagatNo ratings yet
- Respiratory System SummaryDocument6 pagesRespiratory System SummaryKiara GovenderNo ratings yet
- FCE TestDocument10 pagesFCE TestNguyen TrangNo ratings yet
- Inhaler Indentification Guide - 1310 PDFDocument26 pagesInhaler Indentification Guide - 1310 PDFPhanindra Vasu Kotti100% (1)
- Topic 2.1 Ventilatory System Sport Science IBDocument4 pagesTopic 2.1 Ventilatory System Sport Science IBAntonio MouNo ratings yet
- LivingwithcopdbrochureDocument3 pagesLivingwithcopdbrochureapi-676536509No ratings yet
- TOEFL Reading The Wealth of Nations (Answer Key)Document2 pagesTOEFL Reading The Wealth of Nations (Answer Key)eyadNo ratings yet
- ACUTE RESPIRATORY DISTRESSDocument1 pageACUTE RESPIRATORY DISTRESSchristine louise bernardo100% (1)