You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Maintaining Water Quality For Hemodialysis - UpToDateDocument22 pagesMaintaining Water Quality For Hemodialysis - UpToDateRudy Alvarez100% (2)
- NEA Code of Practice For Control of Legionella Bacteria in Cooling TowersDocument33 pagesNEA Code of Practice For Control of Legionella Bacteria in Cooling TowersVishwajeet SinghNo ratings yet
- Puthoff Et Al - Engineering The Zero-Point Field and Polarizable Vacuum For Interstellar Flight (2002)Document8 pagesPuthoff Et Al - Engineering The Zero-Point Field and Polarizable Vacuum For Interstellar Flight (2002)ramy86No ratings yet
- Legionella ToolkitDocument32 pagesLegionella Toolkitilieoniciuc100% (1)
- HANNA General Catalog v28 Chapter10 PhotometersDocument88 pagesHANNA General Catalog v28 Chapter10 PhotometersOrtomet_SANo ratings yet
- Environmental Infection Control in Health-CareDocument249 pagesEnvironmental Infection Control in Health-Caresutheeranand100% (1)
- Australian/New Zealand StandardDocument29 pagesAustralian/New Zealand StandardKayleigh Maynard100% (1)
- EUROHEAT & POWER Guidelines For District Heating SubstationsDocument72 pagesEUROHEAT & POWER Guidelines For District Heating SubstationsVadim Lisnic100% (1)
- Model Cooling Tower Maintenance Program PDFDocument41 pagesModel Cooling Tower Maintenance Program PDFMyo SeinNo ratings yet
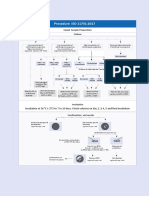
- ISO 11731-2017 Legionella - NewDocument1 pageISO 11731-2017 Legionella - Newsylvana0% (2)
- BS1881-131 1998Document17 pagesBS1881-131 1998venkateswara rao PothinaNo ratings yet
- Legionella Pocket GuideDocument32 pagesLegionella Pocket GuideIoR100% (1)
- Design OTDocument7 pagesDesign OTyafetNo ratings yet
- Title: Intrinsic Safety Made Easy: Profile of Kuan Teik HuaDocument14 pagesTitle: Intrinsic Safety Made Easy: Profile of Kuan Teik Huaramy86No ratings yet
- Recent Developments in Eddy Viscosity Modelling of TurbulenceDocument11 pagesRecent Developments in Eddy Viscosity Modelling of Turbulenceramy86No ratings yet
- Type 262K FilterDocument4 pagesType 262K Filterramy86No ratings yet
- Conservation Laws of Fluid Motion and Boundary Conditions: Ibrahim SezaiDocument20 pagesConservation Laws of Fluid Motion and Boundary Conditions: Ibrahim Sezairamy86No ratings yet
- The Benchtop: A Useful But Little-Known Tool For Science and EngineeringDocument3 pagesThe Benchtop: A Useful But Little-Known Tool For Science and Engineeringramy86No ratings yet
- 951 Eng PerfmodDocument126 pages951 Eng Perfmodramy86No ratings yet
- CTRCTRC TVTRCVT YtvtcvtDocument8 pagesCTRCTRC TVTRCVT Ytvtcvtramy86No ratings yet
- 34536653Document32 pages34536653ramy86No ratings yet
- 944 Turbo Engine Performance ModificationsDocument13 pages944 Turbo Engine Performance Modificationsramy86No ratings yet
- Cvalt PDFDocument2 pagesCvalt PDFramy86No ratings yet
- Laplace Transform InputsDocument4 pagesLaplace Transform Inputsramy86No ratings yet
- Training Attendance Sheet: Committee MentorDocument2 pagesTraining Attendance Sheet: Committee Mentorramy86No ratings yet
- Sanitization-Remove Hidden Data From PDF Files With Adobe Acrobat XIDocument1 pageSanitization-Remove Hidden Data From PDF Files With Adobe Acrobat XIramy86No ratings yet
- A New Hybrid Thermal Comfort Guideline For The Netherlands (ISSO 74: 2014)Document12 pagesA New Hybrid Thermal Comfort Guideline For The Netherlands (ISSO 74: 2014)ramy86No ratings yet
- Incompressible Navier-Stokes RequirementsDocument13 pagesIncompressible Navier-Stokes Requirementsramy86No ratings yet
- Sensormount: SKF Spherical Rolling Bearings and Carb Pioneers in Digital Drive-Up MonitoringDocument2 pagesSensormount: SKF Spherical Rolling Bearings and Carb Pioneers in Digital Drive-Up Monitoringramy86No ratings yet
- Dresser-Rand Engineer Writes Comprehensive Guide To Dry Gas SealsDocument1 pageDresser-Rand Engineer Writes Comprehensive Guide To Dry Gas Sealsramy86No ratings yet
- Compressor Start Up ChecklistDocument2 pagesCompressor Start Up Checklistramy86No ratings yet
- Cloud& Pour Points in Fuel BlendsDocument5 pagesCloud& Pour Points in Fuel Blendsramy86No ratings yet
- Temperature Scales: Visit The Peak Sensors Online Design Guide atDocument1 pageTemperature Scales: Visit The Peak Sensors Online Design Guide atramy86No ratings yet
- GSCP Environmental Reference RequirementsDocument25 pagesGSCP Environmental Reference RequirementsSri KumarNo ratings yet
- Lovibond CatalogDocument96 pagesLovibond CatalogsijinjoyNo ratings yet
- Chlorine Dioxide Generation Bluesense Oxiblu: A Breakthrough in Without PrecursorsDocument29 pagesChlorine Dioxide Generation Bluesense Oxiblu: A Breakthrough in Without PrecursorsMax JunghannsNo ratings yet
- Presentation HuwaSan WT Legionella - CovidDocument22 pagesPresentation HuwaSan WT Legionella - CovidHersh F. HawramyNo ratings yet
- Care Free Water Conditioners EnglishDocument12 pagesCare Free Water Conditioners Englishteguh santosoNo ratings yet
- Biocide BrochureDocument24 pagesBiocide BrochureshalabyahmedNo ratings yet
- Ib 5Document49 pagesIb 5kanishkaNo ratings yet
- Mahon CompileDocument13 pagesMahon CompileSheinor Fae GalzoteNo ratings yet
- WHO Guidelines For Drinking-Water QualityDocument595 pagesWHO Guidelines For Drinking-Water QualityAbdul SalamNo ratings yet
- Drinking Water Parameter Cooperation ProjectDocument240 pagesDrinking Water Parameter Cooperation ProjectramNo ratings yet
- CH 18 Haemophilus and Other Fastidious GNBDocument37 pagesCH 18 Haemophilus and Other Fastidious GNBshericeNo ratings yet
- CoP - 12.0 - Prevention and Control of Legionnaires DiseaseDocument11 pagesCoP - 12.0 - Prevention and Control of Legionnaires DiseaseNiel Brian VillarazoNo ratings yet
- Biofilm Formation On Copper and Galvanized Steel Surfaces in ADocument7 pagesBiofilm Formation On Copper and Galvanized Steel Surfaces in AMarcus ViníciusNo ratings yet
- Equipos Monitoreo de CondicionesDocument11 pagesEquipos Monitoreo de CondicionesJonathan Vasquez LlagunoNo ratings yet
- HuwaSan Brochure PDFDocument8 pagesHuwaSan Brochure PDFKaneki KenNo ratings yet
- Wedeco Sogutma Suyunda Ozon SistemleriDocument8 pagesWedeco Sogutma Suyunda Ozon SistemleriAndrey GyrychNo ratings yet
- Quincy Legionella Report 4-6-18Document35 pagesQuincy Legionella Report 4-6-18Mark MaxwellNo ratings yet
- Spa LegionDocument4 pagesSpa LegionGeorge GeorgievNo ratings yet