You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- National Conference On Co-Operative Societies, Trusts, Organized by Institute of Chartered Accountants of India - Cell Tower Radiation Hazards and SolutionsDocument290 pagesNational Conference On Co-Operative Societies, Trusts, Organized by Institute of Chartered Accountants of India - Cell Tower Radiation Hazards and SolutionsNeha KumarNo ratings yet
- NESA Shielding Product BrochureDocument12 pagesNESA Shielding Product BrochureNeha KumarNo ratings yet
- Cell Phone / Cell Tower Radiation Hazards and SolutionsDocument35 pagesCell Phone / Cell Tower Radiation Hazards and SolutionsNeha KumarNo ratings yet
- Comments On "DOT Report For Allahabad HC" On EMF Radiation and Health - by Prof. Girish KumarDocument70 pagesComments On "DOT Report For Allahabad HC" On EMF Radiation and Health - by Prof. Girish KumarNeha KumarNo ratings yet
- Prof. Girish Kumar's Comments On The Book - "Mobile Phones and Public Health - Myths and Reality"Document10 pagesProf. Girish Kumar's Comments On The Book - "Mobile Phones and Public Health - Myths and Reality"Neha KumarNo ratings yet
- List of Illegal MobileTower - BMCDocument197 pagesList of Illegal MobileTower - BMCNeha KumarNo ratings yet
- Neha Kumar's Story (Director of NESA Radiation Solutions) in Chitralekha Magazine May 2014 IssueDocument2 pagesNeha Kumar's Story (Director of NESA Radiation Solutions) in Chitralekha Magazine May 2014 IssueNeha KumarNo ratings yet
- Cell Tower Radiation and Environment - RASRANG, Dainik BhaskarDocument1 pageCell Tower Radiation and Environment - RASRANG, Dainik BhaskarNeha KumarNo ratings yet
- National Conference Organized by ICAI - Cell Tower Radiation HazardsDocument290 pagesNational Conference Organized by ICAI - Cell Tower Radiation HazardsNeha KumarNo ratings yet
- National Conference On Co-Operative Societies, Trusts, Organized by Institute of Chartered Accountants of India - Cell Tower Radiation Hazards and SolutionsDocument290 pagesNational Conference On Co-Operative Societies, Trusts, Organized by Institute of Chartered Accountants of India - Cell Tower Radiation Hazards and SolutionsNeha KumarNo ratings yet
- Guideline of The Austrian Medical Association For The Diagnosis and Treatment of EMF - Related Health Problems and Illnesses (EMF Syndrome)Document17 pagesGuideline of The Austrian Medical Association For The Diagnosis and Treatment of EMF - Related Health Problems and Illnesses (EMF Syndrome)Neha Kumar100% (1)
- Mobile Tower and Mobile Phone Radiation Hazards - Prof Girish Kumar - June 2013Document50 pagesMobile Tower and Mobile Phone Radiation Hazards - Prof Girish Kumar - June 2013Neha Kumar100% (1)
- Cell Tower Radiation Report by Prof. Girish Kumar - Dec 2012Document45 pagesCell Tower Radiation Report by Prof. Girish Kumar - Dec 2012Neha Kumar100% (1)
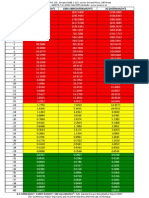
- Conversion Chart For Power Density Reading From DBM To Milli Watt /square Meter (For Frequency 800 MHZ - 4GHz)Document1 pageConversion Chart For Power Density Reading From DBM To Milli Watt /square Meter (For Frequency 800 MHZ - 4GHz)Neha KumarNo ratings yet
- REPLY TO - Comments On Prof Girish Kumar's Presentation On Cell Tower Radiation at ASSOCHAMDocument72 pagesREPLY TO - Comments On Prof Girish Kumar's Presentation On Cell Tower Radiation at ASSOCHAMNeha KumarNo ratings yet
- Workshop On Cell Tower Radiation - Delhi - Agenda of Conference)Document3 pagesWorkshop On Cell Tower Radiation - Delhi - Agenda of Conference)Neha KumarNo ratings yet
- Contributions of WhoDocument6 pagesContributions of WhoRahilNo ratings yet
- Obat Anestesi Intravena: Obat Untuk Dosis OOA DOADocument1 pageObat Anestesi Intravena: Obat Untuk Dosis OOA DOAdede rianiNo ratings yet
- งานเคมีบ าบัด กลุ่มงานเภสัชกรรม โรงพยาบาลราชวิถี ตาราง การเตรียมยา และความคงตัวของยาเคมีบ าบัด Reconstitution PreparationDocument11 pagesงานเคมีบ าบัด กลุ่มงานเภสัชกรรม โรงพยาบาลราชวิถี ตาราง การเตรียมยา และความคงตัวของยาเคมีบ าบัด Reconstitution Preparationtotoil22No ratings yet
- Coronavirus Disease 2019 (COVID-19) : A Cross-Sectional Survey of The Knowledge, Attitudes, Practices (KAP) and Misconceptions in The General Population of Katsina State, NigeriaDocument14 pagesCoronavirus Disease 2019 (COVID-19) : A Cross-Sectional Survey of The Knowledge, Attitudes, Practices (KAP) and Misconceptions in The General Population of Katsina State, NigeriaUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Group 4 Research Paper1Document38 pagesGroup 4 Research Paper1Ana Veia RuizNo ratings yet
- Laporan Apotek Rawat Jalan Juni 2023 2Document122 pagesLaporan Apotek Rawat Jalan Juni 2023 2Pafi AbdyaNo ratings yet
- Bukti Evaluasi Ketersediaan Obat Puskesmas Dengan Formularium PuskesmasDocument29 pagesBukti Evaluasi Ketersediaan Obat Puskesmas Dengan Formularium PuskesmasEghi F MNo ratings yet
- Questionnaire ENG EMRODocument13 pagesQuestionnaire ENG EMROIqra shakeelNo ratings yet
- FAQ Preventing ViolenceDocument12 pagesFAQ Preventing ViolenceCharlesNo ratings yet
- MHGap Intervention Guide PDFDocument107 pagesMHGap Intervention Guide PDFfundj22100% (1)
- Baharain - NHRA-PPR - 2014 Drug Price List - 08!06!2014Document320 pagesBaharain - NHRA-PPR - 2014 Drug Price List - 08!06!2014Anuj MairhNo ratings yet
- Drugs Used in PregnancyDocument1 pageDrugs Used in PregnancyFahad AlkenaniNo ratings yet
- ED Produk KF - KF (Nama Apotek)Document19 pagesED Produk KF - KF (Nama Apotek)Eko FebryandiNo ratings yet
- Canamed 2011Document5,256 pagesCanamed 2011Alina IamandiNo ratings yet
- Eg0993889 1667779185472Document2 pagesEg0993889 1667779185472Adam KamalNo ratings yet
- 1 Covid ResearchDocument89 pages1 Covid ResearchSushmita SolankiNo ratings yet
- Management of Healthcare Waste in UgandaDocument93 pagesManagement of Healthcare Waste in UgandaMohammed NabeelNo ratings yet
- 3RD Quarterly Exam in Mapeh 10Document8 pages3RD Quarterly Exam in Mapeh 10rose ann valleNo ratings yet
- STOK250921Document36 pagesSTOK250921Martha AdinataNo ratings yet
- MCN National HealthDocument4 pagesMCN National HealthCamille RamosNo ratings yet
- A WGIHR2 6-EnDocument197 pagesA WGIHR2 6-EnAzri 2906No ratings yet
- Surat Pesanan APL Okt 18Document234 pagesSurat Pesanan APL Okt 18Eko EdgarNo ratings yet
- Work Immersion Lecture 1 - Health Care SystemDocument9 pagesWork Immersion Lecture 1 - Health Care SystemAMIRA MARIE FERNANDEZNo ratings yet
- (DOH HPB) Orientation To Healthy Learning Institutions and The 2023 HLI ExpansionDocument66 pages(DOH HPB) Orientation To Healthy Learning Institutions and The 2023 HLI ExpansionMark Jason MendozaNo ratings yet
- Albendazole 400 MG: NO Nama Obat Harga Sisa Tanggal ExpiredDocument6 pagesAlbendazole 400 MG: NO Nama Obat Harga Sisa Tanggal ExpiredKlinik PKBI AcehNo ratings yet
- Module 1 Overview of Public Health Nursing in The PhilippinesDocument4 pagesModule 1 Overview of Public Health Nursing in The PhilippinesJJ VeranoNo ratings yet
- TGP Bamban Inventory FormDocument78 pagesTGP Bamban Inventory FormMichael LayugNo ratings yet
- DAFTAR HARGA PT. Kimia FarmaDocument29 pagesDAFTAR HARGA PT. Kimia FarmaAuliaNo ratings yet
- Anti Bio TikaDocument5 pagesAnti Bio TikanunungNo ratings yet
- My Abilities First: Positive Language in Health Care: Disruptive EducationDocument3 pagesMy Abilities First: Positive Language in Health Care: Disruptive EducationVe SaNo ratings yet