You might also like
- In-House Vs Out-Sourced Clinical EngineeringDocument3 pagesIn-House Vs Out-Sourced Clinical EngineeringRino FerdianNo ratings yet
- Shared Services For HealthcareDocument9 pagesShared Services For HealthcareNeeraj SabhnaniNo ratings yet
- Cost EffectivenessDocument8 pagesCost EffectivenessMehul LakhaniNo ratings yet
- Case AnalysisDocument11 pagesCase AnalysisShuchi BhatnagarNo ratings yet
- Operations Management Helps Companies Plan Every Single Aspect of The Business IncludingDocument2 pagesOperations Management Helps Companies Plan Every Single Aspect of The Business IncludingZannatun NayeemNo ratings yet
- Why Do Organizations Outsource?: Human Resources Payroll Processing Facility ManagementDocument6 pagesWhy Do Organizations Outsource?: Human Resources Payroll Processing Facility ManagementAmy GordonNo ratings yet
- Seven Steps of Telehealth PlanningDocument6 pagesSeven Steps of Telehealth PlanningHemprasad BadgujarNo ratings yet
- 10 Necessary ToolsDocument8 pages10 Necessary ToolsNofeestickets AmericaNo ratings yet
- Faculty of Civil Engineering: Sample of Good AssignmentDocument19 pagesFaculty of Civil Engineering: Sample of Good AssignmentJules MoujingNo ratings yet
- ACCT3251 - T00059570 - Ankit Sharma - A5Document14 pagesACCT3251 - T00059570 - Ankit Sharma - A5ANKIT SHARMANo ratings yet
- Brochure NewDocument10 pagesBrochure NewManoj RanaweeraNo ratings yet
- Group 3 Presentation Prince Muzonzini (C19138812H) Marilyne T Sigauke (C19138638G)Document13 pagesGroup 3 Presentation Prince Muzonzini (C19138812H) Marilyne T Sigauke (C19138638G)Jeremiah NcubeNo ratings yet
- Leveraging Healthcare It To Improve Operational PerformanceDocument5 pagesLeveraging Healthcare It To Improve Operational Performancejeric redillasNo ratings yet
- Hca270 Final PresentationDocument12 pagesHca270 Final PresentationJennifer Reynolds100% (2)
- Lead While Serving: An Integrated Approach to Managing Your Stakeholders and CustomersFrom EverandLead While Serving: An Integrated Approach to Managing Your Stakeholders and CustomersNo ratings yet
- Healthcare Terminal Brochure - 112411Document6 pagesHealthcare Terminal Brochure - 112411iyad.alsabiNo ratings yet
- Healthcare Revenue Cycle ManagementDocument6 pagesHealthcare Revenue Cycle ManagementE-Rad Imaging and Reporting services Pvt LtdNo ratings yet
- ManCon - Green Valley (Final Draft)Document13 pagesManCon - Green Valley (Final Draft)Jerome Luna Tarranza100% (1)
- Accenture Returns RepairsDocument7 pagesAccenture Returns RepairsBhairav MehtaNo ratings yet
- Budget Proposal..Final..14.3.11Document12 pagesBudget Proposal..Final..14.3.11Naveen EldoseNo ratings yet
- Quality ImprovementDocument1 pageQuality ImprovementFulgene WandagNo ratings yet
- Chief Information Officer CIO in Southeast USA Resume Joseph WoodDocument3 pagesChief Information Officer CIO in Southeast USA Resume Joseph WoodJosephWoodNo ratings yet
- VP Health Insurance Operations in Boston MA Resume Thomas EverettDocument2 pagesVP Health Insurance Operations in Boston MA Resume Thomas EverettThomas EverettNo ratings yet
- OMBC 204 Unit 1 - 13 Self Assessment MCQsDocument39 pagesOMBC 204 Unit 1 - 13 Self Assessment MCQsPriyanka MahajanNo ratings yet
- Lean Management Tools: Presented By: Theresa Moore Thedacare Improvement SystemDocument42 pagesLean Management Tools: Presented By: Theresa Moore Thedacare Improvement SystemPradeep Poornishankar PNo ratings yet
- Is It Time To Outsource Your Billing?: Joe Macies, Ceo Virtual Officeware Healthcare SolutionsDocument20 pagesIs It Time To Outsource Your Billing?: Joe Macies, Ceo Virtual Officeware Healthcare SolutionsShishir MishraNo ratings yet
- Hospital CEO Best Practices: A Ab BSST TR Ra Ac CT TDocument6 pagesHospital CEO Best Practices: A Ab BSST TR Ra Ac CT Tfrancisco_expósitoNo ratings yet
- Boston Children ProjectDocument2 pagesBoston Children ProjectPankhuri BhatnagarNo ratings yet
- Dissertation On ABC CostingDocument7 pagesDissertation On ABC CostingBuyingPapersSingapore100% (1)
- Medical Billing Resume ExamplesDocument7 pagesMedical Billing Resume Examplesbcr7r579100% (2)
- Issue Diagnosis Memo DRAFT (Djenane Spence AndreDocument5 pagesIssue Diagnosis Memo DRAFT (Djenane Spence Andrewilgens valmyNo ratings yet
- Whitepaper-Insourcing Vs OutsourcingDocument5 pagesWhitepaper-Insourcing Vs OutsourcingRodolfo GloriaNo ratings yet
- Service Operations NotesDocument5 pagesService Operations NotesSanket ShetyeNo ratings yet
- What Constitutes WorldDocument10 pagesWhat Constitutes WorldDiah Indriani KusbandariNo ratings yet
- Case For PS Stakeholder CommDocument19 pagesCase For PS Stakeholder CommRia Tiglao FortugalizaNo ratings yet
- Final Exam 2020-With SoluationsDocument6 pagesFinal Exam 2020-With SoluationsIbrahim Elmorsy Maintenance - 3397No ratings yet
- McKinsey 7-S FrameworkDocument22 pagesMcKinsey 7-S FrameworkShubham GuptaNo ratings yet
- Castlight HealthDocument7 pagesCastlight HealthshardullavandeNo ratings yet
- Summary of Performance IndicatorsDocument4 pagesSummary of Performance IndicatorsgorayjunkNo ratings yet
- How to Enhance Productivity Under Cost Control, Quality Control as Well as Time, in a Private or Public OrganizationFrom EverandHow to Enhance Productivity Under Cost Control, Quality Control as Well as Time, in a Private or Public OrganizationNo ratings yet
- Term Paper Topics On Management AccountingDocument8 pagesTerm Paper Topics On Management Accountingafdtyaxfv100% (1)
- These Are Examples Where You Can Base Your Business Case This Is Not A Complete DocumentDocument12 pagesThese Are Examples Where You Can Base Your Business Case This Is Not A Complete DocumentCyLo PatricioNo ratings yet
- Textbook of Urgent Care Management: Chapter 12, Pro Forma Financial StatementsFrom EverandTextbook of Urgent Care Management: Chapter 12, Pro Forma Financial StatementsNo ratings yet
- E BusinessDocument15 pagesE BusinessGaurav AnandNo ratings yet
- Billing Service: What To Look For When Selecting A Billing ServiceDocument7 pagesBilling Service: What To Look For When Selecting A Billing ServicezahidmNo ratings yet
- Athenahealth: Possible ERP System Modules and Its Features or CharacteristicsDocument3 pagesAthenahealth: Possible ERP System Modules and Its Features or CharacteristicsMaica Joules MontehermosoNo ratings yet
- Tarek Isteak Tonmoy-2016010000130 PDFDocument7 pagesTarek Isteak Tonmoy-2016010000130 PDFTarek Isteak TonmoyNo ratings yet
- Ch03 - Breakeven SolutionDocument42 pagesCh03 - Breakeven SolutionSana Khan0% (1)
- The Outsourcing Revolution (Review and Analysis of Corbett's Book)From EverandThe Outsourcing Revolution (Review and Analysis of Corbett's Book)No ratings yet
- Introduction To CphimsDocument32 pagesIntroduction To Cphimsvkwadhwa01No ratings yet
- 9 Key Strategies To Minimize The Cost of Poor Quality - Insights PDFDocument6 pages9 Key Strategies To Minimize The Cost of Poor Quality - Insights PDFAlsayed DiabNo ratings yet
- BLG CD 030719 2 Inity R1N R2N CNDocument5 pagesBLG CD 030719 2 Inity R1N R2N CNGladstone SamuelNo ratings yet
- Case Study: High Ridge Family PracticeDocument2 pagesCase Study: High Ridge Family PracticemckessonphysicianpracticeNo ratings yet
- Outsourcing in Healthcare IndustryDocument5 pagesOutsourcing in Healthcare IndustryRahul BhagatNo ratings yet
- Director Property Casualty Insurance in Boston MA Resume William KratchDocument2 pagesDirector Property Casualty Insurance in Boston MA Resume William KratchWilliamKratchNo ratings yet
- TQMDocument6 pagesTQMHamza Dawid HamidNo ratings yet
- Ten Critical Steps For A Successful Telemedicine Program: Step #1: Establish A VisionDocument10 pagesTen Critical Steps For A Successful Telemedicine Program: Step #1: Establish A Visionjohn-brownlee-1084No ratings yet
- Distinguish Between Production Management and Operation Management. What Is Production Management?Document13 pagesDistinguish Between Production Management and Operation Management. What Is Production Management?Desu mekonnenNo ratings yet
- Jenny KilburnDocument6 pagesJenny KilburnBrandon Brans NyakoorahNo ratings yet
- REPORT-Investigation Report (Italian Ministry of Infrastructures & Tranports)Document181 pagesREPORT-Investigation Report (Italian Ministry of Infrastructures & Tranports)haloutsoNo ratings yet
- Unlocking The Mask-Process by Which Authentic Leaders Impact FollowersDocument23 pagesUnlocking The Mask-Process by Which Authentic Leaders Impact FollowershaloutsoNo ratings yet
- Authentic Leadership, Creativity & InnovationDocument16 pagesAuthentic Leadership, Creativity & InnovationhaloutsoNo ratings yet
- Luthans-2002-Journal of Organizational BehaviorDocument12 pagesLuthans-2002-Journal of Organizational BehaviorhaloutsoNo ratings yet
- The Equity-Equality ConflictDocument8 pagesThe Equity-Equality ConflicthaloutsoNo ratings yet
- Blood Angels Ref SheetsDocument4 pagesBlood Angels Ref SheetsAndrew ThomasNo ratings yet
- SDM Case Analysis Stihl IncorporatedDocument17 pagesSDM Case Analysis Stihl Incorporatedmahtaabk100% (5)
- Travisa India ETA v5Document4 pagesTravisa India ETA v5Chamith KarunadharaNo ratings yet
- Shop Decjuba White DressDocument1 pageShop Decjuba White DresslovelyNo ratings yet
- Adobe Scan 03-May-2021Document22 pagesAdobe Scan 03-May-2021Mohit RanaNo ratings yet
- Organizational Behavior: Chapter 6: Understanding Work TeamDocument6 pagesOrganizational Behavior: Chapter 6: Understanding Work TeamCatherineNo ratings yet
- How To Write A Driving School Business Plan: Executive SummaryDocument3 pagesHow To Write A Driving School Business Plan: Executive SummaryLucas Reigner KallyNo ratings yet
- RwservletDocument2 pagesRwservletsallyNo ratings yet
- Eicher HR PoliciesDocument23 pagesEicher HR PoliciesNakul100% (2)
- Ekotoksikologi Kelautan PDFDocument18 pagesEkotoksikologi Kelautan PDFMardia AlwanNo ratings yet
- Beowulf Essay 1Document6 pagesBeowulf Essay 1api-496952332No ratings yet
- PAPER 2 RevisedDocument36 pagesPAPER 2 RevisedMâyúř PäťîĺNo ratings yet
- Starmada House RulesDocument2 pagesStarmada House Ruleshvwilson62No ratings yet
- CDR Questionnaire Form: of The Project I.E. How The Objectives of The Project Was Accomplished in Brief.)Document2 pagesCDR Questionnaire Form: of The Project I.E. How The Objectives of The Project Was Accomplished in Brief.)NASEER AHMAD100% (1)
- Consolidated Terminals Inc V Artex G R No L 25748 PDFDocument1 pageConsolidated Terminals Inc V Artex G R No L 25748 PDFCandelaria QuezonNo ratings yet
- Quiet Time Guide 2009Document2 pagesQuiet Time Guide 2009Andrew Mitry100% (1)
- eLTE5.0 DBS3900 Product Description (3GPP)Document37 pageseLTE5.0 DBS3900 Product Description (3GPP)Wisut MorthaiNo ratings yet
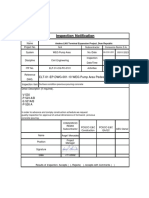
- In-CIV-201 INSPECTION NOTIFICATION Pre-Pouring Concrete WEG Pump Area PedestalsDocument5 pagesIn-CIV-201 INSPECTION NOTIFICATION Pre-Pouring Concrete WEG Pump Area PedestalsPedro PaulinoNo ratings yet
- Albanian DialectsDocument5 pagesAlbanian DialectsMetaleiroNo ratings yet
- GR - 211015 - 2016 Cepalco Vs Cepalco UnionDocument14 pagesGR - 211015 - 2016 Cepalco Vs Cepalco UnionHenteLAWcoNo ratings yet
- Kaalabhiravashtakam With English ExplainationDocument2 pagesKaalabhiravashtakam With English ExplainationShashanka KshetrapalasharmaNo ratings yet
- 10th Grade SAT Vocabulary ListDocument20 pages10th Grade SAT Vocabulary ListMelissa HuiNo ratings yet
- Savage Worlds - Space 1889 - London Bridge Has Fallen Down PDFDocument29 pagesSavage Worlds - Space 1889 - London Bridge Has Fallen Down PDFPablo Franco100% (6)
- Glossary of Important Islamic Terms-For CourseDocument6 pagesGlossary of Important Islamic Terms-For CourseibrahimNo ratings yet
- Relative Clauses: A. I Didn't Know You Only Had OnecousinDocument3 pagesRelative Clauses: A. I Didn't Know You Only Had OnecousinShanti AyudianaNo ratings yet
- Comprehensive Problem Excel SpreadsheetDocument23 pagesComprehensive Problem Excel Spreadsheetapi-237864722100% (3)
- Unit Test 11 PDFDocument1 pageUnit Test 11 PDFYONo ratings yet
- UFC 3-270-01 Asphalt Maintenance and Repair (03!15!2001)Document51 pagesUFC 3-270-01 Asphalt Maintenance and Repair (03!15!2001)Bob VinesNo ratings yet
- Dda 2020Document32 pagesDda 2020GetGuidanceNo ratings yet
- Abrigo Vs Flores DigestDocument4 pagesAbrigo Vs Flores DigestKatrina GraceNo ratings yet