You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
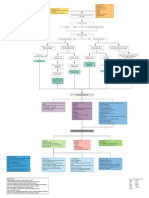
- Myocardial Infarction With CABG Concept MapDocument1 pageMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- Baguio General HospitalDocument2 pagesBaguio General HospitalKatherine NovelaNo ratings yet
- Hydrogen Peroxide TherapyDocument0 pagesHydrogen Peroxide TherapyGetto Vocab100% (2)
- Methods RM ModuleDocument36 pagesMethods RM ModuleAnonymous iqoU1mtNo ratings yet
- Prognostic Relevance of The Expression of TDT and CD7 in 335 Cases of Acute Myeloid LeukemiaDocument8 pagesPrognostic Relevance of The Expression of TDT and CD7 in 335 Cases of Acute Myeloid LeukemiaAnonymous iqoU1mtNo ratings yet
- 4 A Retrospective ReflectionDocument16 pages4 A Retrospective ReflectionAnonymous iqoU1mtNo ratings yet
- Pallikaranai Margazhi ThiruvizhaDocument3 pagesPallikaranai Margazhi ThiruvizhaAnonymous iqoU1mtNo ratings yet
- Alpha-Gal Detectors in Xenotransplantation Research: A Word of CautionDocument6 pagesAlpha-Gal Detectors in Xenotransplantation Research: A Word of CautionAnonymous iqoU1mtNo ratings yet
- Biological Evaluation of Medical Devices / Biosafety: Applicable ProductsDocument5 pagesBiological Evaluation of Medical Devices / Biosafety: Applicable ProductsAnonymous iqoU1mtNo ratings yet
- Medical Device RegulationDocument6 pagesMedical Device RegulationAnonymous iqoU1mt100% (2)
- H&E Staining Overview: A Guide To Best Practices:, JD CT (Ascp) HTL, Bappsc, FaimsDocument29 pagesH&E Staining Overview: A Guide To Best Practices:, JD CT (Ascp) HTL, Bappsc, FaimsAnonymous iqoU1mtNo ratings yet
- Artikel SVTDocument17 pagesArtikel SVTbambang hermawanNo ratings yet
- Spiders Nerv SystemDocument3 pagesSpiders Nerv Systemelcrack1231No ratings yet
- Chapter 12 Vasodilators and Angina PectorisDocument7 pagesChapter 12 Vasodilators and Angina PectorisChristine Annmarie TapawanNo ratings yet
- ECG Learning PackageDocument19 pagesECG Learning Packagearulsidd74No ratings yet
- Bio Circulation Sba SumnDocument6 pagesBio Circulation Sba SumnNelicia WilliamsNo ratings yet
- L5 NotesDocument9 pagesL5 Notes17 ERMINO, Nicole AngelaNo ratings yet
- Endothelium: What Is The Basic Structure of Endothelium?Document2 pagesEndothelium: What Is The Basic Structure of Endothelium?Aurelia AlexandraNo ratings yet
- Obs Gynae Presentation by Roll No 127Document23 pagesObs Gynae Presentation by Roll No 127Siddharth KatyalNo ratings yet
- Chapter 31: Structure and Function of The Cardiovascular and Lymphatic SystemsDocument12 pagesChapter 31: Structure and Function of The Cardiovascular and Lymphatic SystemsMelissa WrightNo ratings yet
- 1.enrichment Activities For Respiratory and Circulatory SystemDocument31 pages1.enrichment Activities For Respiratory and Circulatory SystemMarilyn Castro LaquindanumNo ratings yet
- Electrocardiography - Wikipedia, The Free EncyclopediaDocument18 pagesElectrocardiography - Wikipedia, The Free Encyclopediapayments8543No ratings yet
- Human Body Systems VocabularyDocument4 pagesHuman Body Systems Vocabularyapi-231946379No ratings yet
- Mitral Valve ProlapseDocument1 pageMitral Valve ProlapseMindy Leigh LayfieldNo ratings yet
- Solved Problems in Ergonomics 2012Document20 pagesSolved Problems in Ergonomics 2012rianna rose dela cruzNo ratings yet
- Frog DissectionDocument7 pagesFrog DissectionriancfNo ratings yet
- Kelompok 15 PBL 2Document26 pagesKelompok 15 PBL 2Riqah Nefiyanti WardanaNo ratings yet
- Pharmacological Treatment of Acute Coronary Syndromes 2014 PDFDocument260 pagesPharmacological Treatment of Acute Coronary Syndromes 2014 PDFSonoko KurobaNo ratings yet
- CMA Vital Signs Practice Test: Body TemperatureDocument13 pagesCMA Vital Signs Practice Test: Body TemperatureOzgan Süleyman100% (2)
- Wireless Heart Attack Detection SystemDocument3 pagesWireless Heart Attack Detection SystemIJSTENo ratings yet
- Blood Vessels Lecture Slides PDFDocument32 pagesBlood Vessels Lecture Slides PDFRaluca AlexandraNo ratings yet
- 2017 - Diretrizes CMD (European Society of Veterinary Cardiology)Document11 pages2017 - Diretrizes CMD (European Society of Veterinary Cardiology)Flávia PinheiroNo ratings yet
- Final NCPDocument21 pagesFinal NCPkoringring100% (1)
- Dopamine Drug StudyDocument3 pagesDopamine Drug StudyAnne de Vera50% (2)
- 1047Document1,149 pages1047MANG82% (11)
- Journal Heptojugular RefluxDocument5 pagesJournal Heptojugular RefluxFarhan RezaNo ratings yet
- General Principles: Thoracotomy Performed ToDocument4 pagesGeneral Principles: Thoracotomy Performed ToreylaberintoNo ratings yet
- Assessment of Cardiovascular Function Hinkle PPT CH 25Document26 pagesAssessment of Cardiovascular Function Hinkle PPT CH 25DelindaEvans100% (1)