You might also like
- Examination of Body Fluids (Urinalysis)Document109 pagesExamination of Body Fluids (Urinalysis)kiedd_04100% (9)
- Clinical ChemistryDocument26 pagesClinical Chemistryazoooz502No ratings yet
- Intro To Medtech Clinical Chemistry ReviewerDocument11 pagesIntro To Medtech Clinical Chemistry Reviewerjesanndei100% (1)
- 13 Biochemical Tests For Gram Negative Bacilli PDFDocument51 pages13 Biochemical Tests For Gram Negative Bacilli PDFSHUPATUSSAINo ratings yet
- Clinical Bacteriology ReviewerDocument17 pagesClinical Bacteriology Reviewer99noname100% (1)
- Group 4 - General Pathology, Logic and Cytologic TechniquesDocument11 pagesGroup 4 - General Pathology, Logic and Cytologic Techniquesjulo_05No ratings yet
- Antibody IdentificationDocument74 pagesAntibody IdentificationNilver Zenteno100% (3)
- ML7111 MCQs Answers April 2020Document16 pagesML7111 MCQs Answers April 2020Cleo SalvadorNo ratings yet
- Urine Screening of Metabolic DisordersDocument24 pagesUrine Screening of Metabolic DisordersMark Arlo Hernandez SegundoNo ratings yet
- Microscopic Examination of UrineDocument4 pagesMicroscopic Examination of UrineGlaiza Erika Baes GudaNo ratings yet
- Plasma Hemoglobin and Urine Hemoglobin EstimationDocument12 pagesPlasma Hemoglobin and Urine Hemoglobin EstimationAvi VermaNo ratings yet
- Blood Banking Course BookDocument2 pagesBlood Banking Course BookShukr Wesman BlbasNo ratings yet
- Group 8 - Microbiology 1 - BacteriologyDocument14 pagesGroup 8 - Microbiology 1 - Bacteriologyjulo_05No ratings yet
- Analysis of Urine and Other Body FluidsDocument52 pagesAnalysis of Urine and Other Body FluidsJoseph VillamorNo ratings yet
- Urinalysis and Body Fluids2020Document47 pagesUrinalysis and Body Fluids2020MONFOLA100% (1)
- AUBF Analysis of Urine and Body FluidsDocument581 pagesAUBF Analysis of Urine and Body FluidsQuetzaL coatL100% (1)
- SerologyDocument84 pagesSerologyngsusannasuisum100% (2)
- Anticoagulants and Other PreservativesDocument26 pagesAnticoagulants and Other Preservativessdas317No ratings yet
- Stool AnalysisDocument8 pagesStool AnalysisLuciaGomez100% (1)
- Blood Bank ProceduresDocument33 pagesBlood Bank Proceduresninadroy2844100% (20)
- Transfusion Medicine QuestionsDocument31 pagesTransfusion Medicine QuestionsJhoanie Sanggoy Tauli100% (1)
- Clinical Chemistry Review NotesDocument54 pagesClinical Chemistry Review NotesALEONA AMON ARANTENo ratings yet
- Hema I Chapter 7 - HemocytometryDocument83 pagesHema I Chapter 7 - HemocytometryderibewNo ratings yet
- Biochemical Test of BacteriaDocument33 pagesBiochemical Test of Bacteriaaziskf100% (2)
- Group 1 - Analysis of Urine and Other Body FluidsDocument11 pagesGroup 1 - Analysis of Urine and Other Body Fluidsjulo_05100% (3)
- Hematology Ii Lectures Introduction To HemostasisDocument28 pagesHematology Ii Lectures Introduction To HemostasisJoshua Trinidad100% (1)
- Clinical Chemistry: ToxicologyDocument9 pagesClinical Chemistry: ToxicologyChristine BadilloNo ratings yet
- AUB - Urine Screening For Metabolic DisordersDocument3 pagesAUB - Urine Screening For Metabolic DisordersJeanne Rodiño100% (1)
- Lab ValuesDocument5 pagesLab Valuespragya_devkotaNo ratings yet
- LN Hematology MLT FinalDocument549 pagesLN Hematology MLT FinalMahfuzur Rahman100% (3)
- Diagnostic Bacteriology-Lab ReviewDocument45 pagesDiagnostic Bacteriology-Lab ReviewAtiya HajjajNo ratings yet
- Forward and ReverseDocument11 pagesForward and ReversecyrhenmieNo ratings yet
- Clinical Laboratory Science Review by Theriot - JarreauDocument12 pagesClinical Laboratory Science Review by Theriot - JarreauJuneya Koo100% (1)
- Urinalysis and Body Fluids Q & ADocument79 pagesUrinalysis and Body Fluids Q & ADarla YsavelNo ratings yet
- Practice Questions 1Document12 pagesPractice Questions 1Cha100% (1)
- Enterobacter QuizDocument8 pagesEnterobacter QuizDan Paolo Sanchez100% (2)
- Biochemical TestDocument13 pagesBiochemical TestSusi100% (1)
- Blood Grouping TecheniquesDocument19 pagesBlood Grouping TecheniquesLIBIN PALLUPPETTAYIL JOSE93% (15)
- (Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Document16 pages(Microbio) Staphyloccocus and Streptococcus-Dr. Salandanan (BHND)Lee Delos Santos100% (1)
- Laboratory Dha Praparation MCQ 1-2700Document263 pagesLaboratory Dha Praparation MCQ 1-2700Laal Shirt100% (1)
- Donor Screening and Component PreparationDocument91 pagesDonor Screening and Component PreparationDominic BernardoNo ratings yet
- 8.nature of Clinical Laboratory - EditedDocument56 pages8.nature of Clinical Laboratory - EditedJr BalagtasNo ratings yet
- Micro Lab Prac - PDCR PDFDocument10 pagesMicro Lab Prac - PDCR PDFPatti Danielle Referente50% (2)
- Clinical Chemistry Notes With BlanksDocument34 pagesClinical Chemistry Notes With Blanksepson printerNo ratings yet
- Review in Clinical MicrosDocument103 pagesReview in Clinical MicrosSyvelmarie Tinte100% (1)
- Medical Laboratory Science Post Basic CurriculumDocument187 pagesMedical Laboratory Science Post Basic CurriculumNigusse Obse100% (4)
- Analysis of UrineDocument5 pagesAnalysis of UrineHaridha ChandranNo ratings yet
- Histopathology Chapter 2Document141 pagesHistopathology Chapter 2Zelalem Dejazmach100% (2)
- Must To Know MTLDocument15 pagesMust To Know MTLMae MacalandaNo ratings yet
- Hematology Special StainDocument28 pagesHematology Special Stainandreea0dey100% (1)
- CH 1 2 3 4-5-Professional EthicsDocument81 pagesCH 1 2 3 4-5-Professional EthicsAhmadin Bamud100% (1)
- C1 IH Lab L3 ABO Forward Reverse Typing Manual and Gel MethodDocument8 pagesC1 IH Lab L3 ABO Forward Reverse Typing Manual and Gel MethodDIVINA KYLE YGONo ratings yet
- Clinical Microscopy ExamDocument3 pagesClinical Microscopy ExamKarla GiorlaNo ratings yet
- Clinical Microscopy: Definition and Volume Disease and Cause PolyuriaDocument5 pagesClinical Microscopy: Definition and Volume Disease and Cause PolyuriaJovanni andesNo ratings yet
- By: Dr. Yoavita Moderator: Dr. Anik Widijanti, SP - PK (K)Document61 pagesBy: Dr. Yoavita Moderator: Dr. Anik Widijanti, SP - PK (K)Gilang KusdinarNo ratings yet
- Urine ComponentsDocument31 pagesUrine ComponentsLarry MagwegweNo ratings yet
- Urine-Analysis 140420Document74 pagesUrine-Analysis 140420sabao kizuiteNo ratings yet
- Unit 6 UrineDocument131 pagesUnit 6 UrineAsjad HassanNo ratings yet
- URINALYSISDocument80 pagesURINALYSISredr7131No ratings yet
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Document2 pagesIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04No ratings yet
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- The Place For Others in IslamDocument27 pagesThe Place For Others in Islamkiedd_04No ratings yet
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- "Traditional" Exegeses of Q 4:34Document15 pages"Traditional" Exegeses of Q 4:34kiedd_04No ratings yet
- Microbiology Colour Plate No.9Document1 pageMicrobiology Colour Plate No.9kiedd_04No ratings yet
- Fadhilat Surah at TakwirDocument1 pageFadhilat Surah at Takwirkiedd_04No ratings yet
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocument13 pagesOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- SYNAPSEDocument35 pagesSYNAPSEkiedd_04100% (3)
- Cell PhysiologyDocument61 pagesCell Physiologykiedd_04100% (4)
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocument10 pagesPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04No ratings yet
- Microbiology Colour Plate No.3Document1 pageMicrobiology Colour Plate No.3kiedd_04No ratings yet
- Microbiology Colour Plate No.8Document1 pageMicrobiology Colour Plate No.8kiedd_04No ratings yet
- Microbiology Colour Plate No.7Document1 pageMicrobiology Colour Plate No.7kiedd_04No ratings yet
- Microbiology Colour Plate No.2Document1 pageMicrobiology Colour Plate No.2kiedd_04No ratings yet
- Microbiology Colour Plate No.4Document1 pageMicrobiology Colour Plate No.4kiedd_04No ratings yet
- Microbiology Colour Plate No.5Document1 pageMicrobiology Colour Plate No.5kiedd_04No ratings yet
- Microbiology Colour Plate No.6Document1 pageMicrobiology Colour Plate No.6kiedd_04No ratings yet
- API® CoryneDocument4 pagesAPI® Corynekiedd_04No ratings yet
- Microbiology Colour Plate No.1Document1 pageMicrobiology Colour Plate No.1kiedd_04No ratings yet
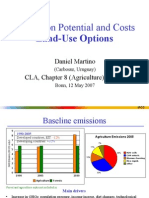
- Mitigation Potential and Costs Land-Use OptionsDocument9 pagesMitigation Potential and Costs Land-Use Optionskiedd_04No ratings yet
- Mitigation of Climate ChangeDocument41 pagesMitigation of Climate Changekiedd_04No ratings yet
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocument1 pageAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)
- Mitigation of Climate ChangeDocument25 pagesMitigation of Climate Changekiedd_04No ratings yet
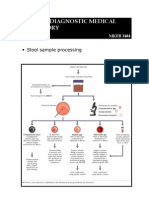
- Stool Sample ProcessingDocument1 pageStool Sample Processingkiedd_04No ratings yet
- Diagram of Classification of EnterobacteriaDocument1 pageDiagram of Classification of Enterobacteriakiedd_04100% (1)
- Oxidase TestDocument1 pageOxidase Testkiedd_04100% (1)
- Carnitine DeficiencyDocument21 pagesCarnitine Deficiencykiedd_04100% (1)
- CAPE Chemistry FormulaeDocument9 pagesCAPE Chemistry FormulaeAmateurVoice LeelaNo ratings yet
- Chapter4 Cost AllocationDocument14 pagesChapter4 Cost AllocationNetsanet BelayNo ratings yet
- People of The Philippines, Plaintiff, vs. Primo Campuhan Y BELLO, Accused. DecisionDocument8 pagesPeople of The Philippines, Plaintiff, vs. Primo Campuhan Y BELLO, Accused. Decisiondiamajolu gaygonsNo ratings yet
- Gas Detector Bump Test Record Log Sheet: Bump Test Result Test Date Time Pass Fail Retest Pass Retest Fail Tester NameDocument2 pagesGas Detector Bump Test Record Log Sheet: Bump Test Result Test Date Time Pass Fail Retest Pass Retest Fail Tester NameAndry Kurnia100% (2)
- Important MCQ Colloction For PartDocument154 pagesImportant MCQ Colloction For PartNazia Ali86% (7)
- Steca TR 0201 Instruction enDocument40 pagesSteca TR 0201 Instruction endaviko313No ratings yet
- RFOC Learner's Guide Page 1-212Document240 pagesRFOC Learner's Guide Page 1-212Travel GnrOneNo ratings yet
- LeRoy v. United States of America - Document No. 3Document5 pagesLeRoy v. United States of America - Document No. 3Justia.comNo ratings yet
- 5000L Series CatalogueDocument24 pages5000L Series CataloguekahlaouiNo ratings yet
- Division of Humanities: Use and Convert To PDF File This Format Every Time You Will Submit Your Activity To VLEDocument3 pagesDivision of Humanities: Use and Convert To PDF File This Format Every Time You Will Submit Your Activity To VLEIane Jhazzlee MapileNo ratings yet
- 10 Suresh Nair - Journey ManagementDocument25 pages10 Suresh Nair - Journey ManagementMuhammad Zulkifli HarahapNo ratings yet
- Fluoroscopy Initial TestDocument3 pagesFluoroscopy Initial Testthepharaoh1234No ratings yet
- Pressure Systems Safety Regulations 2000Document10 pagesPressure Systems Safety Regulations 2000Alberico MuratoriNo ratings yet
- UntitledDocument386 pagesUntitledG PalaNo ratings yet
- Checklist of Eligibility Requirements For Consulting ServicesDocument2 pagesChecklist of Eligibility Requirements For Consulting ServicesAndrea BroccoliNo ratings yet
- Priorities in Critical Care Nursing 7th Edition Urden Test BankDocument35 pagesPriorities in Critical Care Nursing 7th Edition Urden Test Banklief.tanrec.culjd100% (26)
- AGR. 376 - Meat Processing Technology: Beef Fabrication and Identification of Cuts Dr. Stanley F. Kelley Fall 2000Document22 pagesAGR. 376 - Meat Processing Technology: Beef Fabrication and Identification of Cuts Dr. Stanley F. Kelley Fall 2000EugeniuNo ratings yet
- Physics of The Solid Earth (Phy 202)Document11 pagesPhysics of The Solid Earth (Phy 202)Gaaga British0% (1)
- Guidance ProgramDocument4 pagesGuidance ProgramShainajoy BoterNo ratings yet
- Borang IshipDocument9 pagesBorang IshipUlfa RahayuNo ratings yet
- Ownership Data: InstallationDocument2 pagesOwnership Data: InstallationRoshin99No ratings yet
- Quarterly Test - Q3 English 9Document6 pagesQuarterly Test - Q3 English 9Rodrigl BaiganNo ratings yet
- US8236919Document4 pagesUS8236919Billy FowlerNo ratings yet
- George P. Prigatano-Principles of Neuropsychological Rehabilitation PDFDocument375 pagesGeorge P. Prigatano-Principles of Neuropsychological Rehabilitation PDFTlaloc Gonzalez100% (7)
- Pile Hammer Delmag d12-42Document1 pagePile Hammer Delmag d12-42Jorge Rosero QuevedoNo ratings yet
- Leica LS10 LS15 User ManualDocument106 pagesLeica LS10 LS15 User Manualabdelghafour adjNo ratings yet
- 6 Training PlanDocument9 pages6 Training PlanDinesh Kanukollu100% (1)
- The Indian Weekender, Friday 15 May 2020 - Volume 12 Issue 09Document20 pagesThe Indian Weekender, Friday 15 May 2020 - Volume 12 Issue 09Indian Weekender ReporterNo ratings yet
- Article 2194Document9 pagesArticle 2194anhiramdhani100% (1)
- LabreportDocument4 pagesLabreportDarwinys SamijonNo ratings yet