IMPACT: International Journal of Research in Applied, Natural and Social Sciences (IMPACT: IJRANSS) ISSN 2321-8851 Vol.
1, Issue 3, Aug 2013, 87-90 Impact Journals
MULTIPLE XY SYNDROME: A CASE STUDY
ASHMA GUPTA1, PARVINDER KUMAR2, SUBASH GUPTA3 & ABHAY SINGH YADAV4
1,2,3 4
Human Genetic Research cum Counselling Centre, University of Jammu, Jammu, India
Human Cytogenetics Laboratory, Department of Zoology, Kurukshetra University, Kurukshetra, India
ABSTRACT
The present study is an account of the karyotypic analysis carried out in a three and half year old male child born to a young, healthy, non-consanguineous couple. Clinically the child had undescended testes (Cryptorchidism) with empty scrotal sac. It was an uneventful, full term delivery with no family history of congenital anomalies. Besides cryptorchidism, the child had developmental delay as well as mental retardation. Chromosome study was carried out to rule out the chromosomal cause, if any in the child having gross phenotypic anomalies. The karyotype of the child was found to be 49, XXXYY.
KEYWORDS: Cryptorchidism, Developmental Delay, Chromosome Study INTRODUCTION
Sex chromosomal abnormalities especially that of the X-chromosome, have largely been associated with the development of reproductive system, however, abnormalities of the X and Y chromosomes have been held responsible for the birth of Klinefelter syndrome and its variant (Caldwell and Smith 1972; Robinson et al. 1979; Linden et al. 1995; Visootsak et al. 2001; Tartaglia et al. 2011). Although somatic malformations and mental retardation are more severe in the variants of Klinefelter syndrome, Majority of the cases remain undiagnosed till puberty when the clinical symptoms of androgen deficiency get manifested (Purnak et al. 2012). Children born with sex chromosomal abnormalities may have hypospadias, small phallus or cryptorchidism etc., but it is not always a feature of the Klinefelter syndrome and its variants (Lee et al. 2007; Visootsak and Graham 2006). Chromosomal evaluation is, therefore, warranted in all those children born with hypospadias, small phallus or cryptorchidism or any other abnormality of the external genitalia, so as to rule out the sex chromosomal abnormalities in these children.
MATERIALS AND METHODS
Case History Three and half year old clinically diagnosed male child under study had phenotypic anomalies of the external genitalia (Figure 1) along with delayed neuromotor development milestone and mental retardation. To know the status of the testes, the child was subjected to abdominal ultrasonography. Though the testes were found located in the inguinal region and they had not descended in the scrotal sac (Figure 2). As a result of this, the scrotal sacs though had a rouge but they were empty from inside. For cytogenetic study in the child under study, chromosome preparations were obtained from the cultured lymphocytes following the technique of Moorhead et al. (1960). Slides were prepared from the harvested lymphocytes using standard techniques whereas G-banding was done by using 10% trypsin following Benn and Perle (1992). Nearly 2025 well spread metaphase plates were analyzed for ascertaining the chromosome number and a few of these metaphase plates were selected for the preparation of karyotypes using automated cytogenetic workstation (Olympus).
88
Ashma Gupta, Parvinder Kumar, Subash Gupta & Abhay Singh Yadav
Figure 1: Abnormal Genitalia
Figure 2: Abdominal Ultrasonograph Picture
RESULTS AND DISCUSSIONS
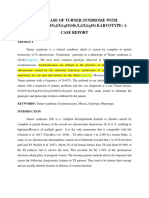
Cytogenetic study in children born with congenital anomalies, including those of the external genitalia, developmental delay and mental retardation becomes important to detect the chromosomal cause for the congenital anomalies and associated abnormalities these children are born with. Well Spread metaphase plates were selected both for finding out the chromosome number and the preparation of karyotypes. Every metaphase plate contained 49 chromosomes i.e. 3 additional chromosomes were present in each one of the metaphase plate (Figure 3). To find out the nature of the additional chromosomes, some of the well spread metaphase plates were karyotyped. Karyotypes prepared were found abnormal as every karyotype contained five sex chromosomes XXXYY suggesting thereby the aneuploidy of both the X and Y chromosomes. Additional X and Y chromosomes were, therefore, held responsible for the congenital anomalies such as cryptorchidism, developmental delay and mental retardation in the child under study. On the basis of the number of X and Y chromosomes, the child was designated as a variant Klinefelter syndrome. Klinefelter syndrome and its variants constitute a group of chromosomal disorder where one or more than one X / Y chromosome is added to the normal male karyotype, 46 XY. Although XXY is the most common karyotype, other karyotypes, though less common having been reported amongst the variants of Klinefelter syndrome are 48, XXYY; 48, XXXY; and 49, XXXYY by Caldwell and Smith (1972); Robinson et al. (1979); Bray and Hosephine (1963); Lecluse-van der Blit et al. (1974); Visootsak and Graham (2006); Linden et al. (1995). The extra X as well as Y chromosome being responsible for the Klinefelter syndrome and its variant are also the leading cause of other phenotypic anomalies such as delayed milestone, mental retardation etc. (Kabra and Gulati 2003; Visootsak and Graham 2003). The extra X chromosome in Klinefelter syndrome and its variants has its origin either from meiotic non-disjunction in male or female gametogenesis whereas the extra Y chromosome arises during male gametogenesis. The likelihood of the extra X has been linked to the advancing maternal age (Visootsak and Graham 2003), but in the present case both the parents were below 30 years of age thus ruling out the influence of parental age on meiotic non-disjunction.
Figure 3: Complement and Karyotype
Multiple XY Syndrome: A Case Study
89
The number of extra X chromosomes do affect the physical as well as mental development as it increases with an increase in the number of X chromosome (Visootsak et al. 2001; Rovet et al. 1995). The case under study also had the delayed physical and mental development that may be attributed to the excess number of X chromosome as well as Y chromosome. Therefore, the more supernumerary sex chromosomes that exist, the more likely are the detrimental physical and mental findings (Chen 2003). Occasionally a finding of the cryptorchidism leads to the diagnosis of XXY child because XXY karyotype is nearly three times more frequent than in this group in the overall population (Topper et al. 1982; Lee et al. 2007) of the sex chromosomal abnormalities 48, XXYY, 49, XXXXY and 49, XXXYY have rarely been reported (Bray and Hosephine 1963; Lecluse-van der Bilt et al. 1974; Ratcliffe and Paul 1986; Robinson et al. 1979) and the present case is an addition to the existing data.
ACKNOWLEDGEMENTS
Authors are thankful to J&K State Council for Science and Technology, Department of Science and Technology, J&K Govt. for providing financial Support to complete the present study.
REFERENCES
1. Benn PA, & Perle MA (1992). Chromosome staining and banding techniques: In: DE Rooney, BH Czepulowski (Eds): Human Cytogenetics. A practical approach. Vol 1: New York: Oxford University Press, Pp. 91-118. 2. 3. Bray P, & Hosephine A (1963). An XXXYY- sex chromosome anomaly. JAMA 184:179. Chen H (2003). Klinefelter Syndrome. Available at: http://www.emedicine. Com/PED/topic 1252 htn. Accessed on August 11. 4. Caldwell PD, & Smith DW, (1972). The XXY (Klinefelters) Syndrome in childhood: detection and treatment. J.Pediatr; 80: 250-258. 5. 6. 7. 8. 9. Kabra M, & Gulati S (2003). Mental retardation. Indian J Pediatr, 70 (2):153-158. Lecluse-van der Bilt FA, et al. (1974). An infant in an XXXYY karyotype. Clin Genet 5:263. Lee YS, et al. (2007). Genetic anomalies in Klinefelter syndrome. Hormone Research 68 (3): 152-5. Linden MG, et al. (1995). Sex chromosome tetrasomy and pentasomy. Pediatrics 96:672-682. Moorhead PS, et al. (1960). Chromosome preparation of leukocytes cultured from human peripheral blood. Experimental Cell Research. 20: 613-616. 10. Purnak Seda, et al. (2012). Diagnosis of variant klinefelter syndrome in 21 year old male who presented with sparse facial hair. Ann Dermatol. 24 ( 3) : 368-369. 11. Rateliffe SG, & Paul N (1986). Prospective studies on sex chromosome aneuploidy. Birth defects. 22 12. Robinson A, Lubs HA, Nielsen J et al. (1979). Summary of clinical findings: Profiles of children with 47, XXY, 47, XXX and 47, XYY Karyotypes. Birth defects 15: 261.
13. Rovet J, Netley C, Bailey J, et al., (1995). Intelligence and achievement in children with extra aneuploidy: A longitudinal perspective. Am J Med Genet; 60: 356- 363. 14. Tartaglia N, Ayari N, Howell S, DEpagnier C, Zeitler P. (2011). 48XXYY, 48 XXXY syndromes: not just variants of Klinefelter syndrome. Acta Paediatr 100: 851-860. and 49XXXXY
90
Ashma Gupta, Parvinder Kumar, Subash Gupta & Abhay Singh Yadav
15. Topper E, Doickerman Z, Prager- Lewinr, Kaufman H, Maimon Z, Laron Z (1982). Puberty in 24 patients with Klinefelter syndrome. Eur J Pediatr: 139: 8-12. 16. Visootsak J, Aylstock M, Graham JH (2001). Klinefelther syndrome and its variants: an update and review for the primary pediatrician. Clin Pediatr 40:639-651. 17. Visootsak Jeannie and Graham M John (2003). Klinefelter syndrome and its variants. Orphanet encyclopedia. March 2003. 18. Visootsak Jeannie and Graham M John (2006). Klinefelter syndrome and other sex chromosomal aneuploidies. Orphanet Journal of Rare diseases 1: 42 d o i: 10: 1186/1750-1172-1-42.
You might also like
- Adya Ebook On Water and MineralsDocument80 pagesAdya Ebook On Water and Mineralsapi-261829418No ratings yet
- Meindl, R.S. Et Al. 1985 Accuracy and Direction of Error in The Sexing of The SkeletonDocument7 pagesMeindl, R.S. Et Al. 1985 Accuracy and Direction of Error in The Sexing of The SkeletonElen FeuerriegelNo ratings yet
- Intro To Mycology Prelims2Document47 pagesIntro To Mycology Prelims2Annika AbadNo ratings yet
- The Crystal PalaceDocument11 pagesThe Crystal PalaceBlessedmartyrNo ratings yet
- Evidence Supporting The Biological Nature of Gender IdentityDocument6 pagesEvidence Supporting The Biological Nature of Gender IdentityMorgan Atwood100% (2)
- Ring Chromosome 13 and Ambiguous GenitaliaDocument3 pagesRing Chromosome 13 and Ambiguous Genitaliakaychi zNo ratings yet
- Intersex or Disorders of Sexual DevelopmentDocument19 pagesIntersex or Disorders of Sexual DevelopmentHUSAMNo ratings yet
- Klinefelter Syndrome and Associated Fragile-X Syndrome: Case II-5Document8 pagesKlinefelter Syndrome and Associated Fragile-X Syndrome: Case II-5صادقNo ratings yet
- Fate of SRY, PABY, DYS1, DYZ3 and DYZ1 loci in sex chromosomal anomalies patientsDocument11 pagesFate of SRY, PABY, DYS1, DYZ3 and DYZ1 loci in sex chromosomal anomalies patientsrenny100% (1)
- NANTHINIDocument28 pagesNANTHINIADHITHIYA VNo ratings yet
- Microduplication of xp22.31Document4 pagesMicroduplication of xp22.31Roberth SanchezNo ratings yet
- Ambiguous Fonda Full Icomesh3Document20 pagesAmbiguous Fonda Full Icomesh3share fosNo ratings yet
- EVIDENCE SUPPORTING BIO NATURE OF GENDER IDENTITY - Saraswat & SaferDocument20 pagesEVIDENCE SUPPORTING BIO NATURE OF GENDER IDENTITY - Saraswat & Safercrosskeys001No ratings yet
- Clinical, Biological and Genetic Analysis of Anorchia in 26 BoysDocument5 pagesClinical, Biological and Genetic Analysis of Anorchia in 26 Boysarda_ccerNo ratings yet
- Biological Theories of Gender: HormonesDocument8 pagesBiological Theories of Gender: HormonesDanica De VeraNo ratings yet
- Sex and Congenital Diaphragmatic Hernia: OriginalarticleDocument5 pagesSex and Congenital Diaphragmatic Hernia: OriginalarticleBlank SpaceNo ratings yet
- Michelle - Entonu.sbi4u BioethicsDocument5 pagesMichelle - Entonu.sbi4u Bioethicsmichelleentonu326No ratings yet
- A Case Study About Klinefelter SyndromeDocument6 pagesA Case Study About Klinefelter Syndromehoy100% (1)
- Burégio-Frota Et Al 2010Document5 pagesBurégio-Frota Et Al 2010dida_bispoNo ratings yet
- Low Rates of Pregnancy Termination For Prenatally Diagnosed Klinefelter Syndrome and Other Sex Chromosome PolysomiesDocument5 pagesLow Rates of Pregnancy Termination For Prenatally Diagnosed Klinefelter Syndrome and Other Sex Chromosome PolysomiesAltaicaNo ratings yet
- 47, XYY Syndrome and Its Association With Male Infertility: CaseDocument3 pages47, XYY Syndrome and Its Association With Male Infertility: CaseprasadbheemNo ratings yet
- Ambiguous Genitalia 3Document4 pagesAmbiguous Genitalia 3syarifah salmaNo ratings yet
- 6 Gender Atypical Gender DevelopmentDocument9 pages6 Gender Atypical Gender DevelopmentFN IS MOISTNo ratings yet
- Genetic Disorder Fact SheetDocument3 pagesGenetic Disorder Fact SheetPreethy JayNo ratings yet
- Prenatal Diagnosis of Sex Differentiation DisorderDocument8 pagesPrenatal Diagnosis of Sex Differentiation DisorderHorvath AlexandraNo ratings yet
- Arumugam Et Al-Clinical Anatomy 2Document10 pagesArumugam Et Al-Clinical Anatomy 2Kavitha RajaNo ratings yet
- Expression of Estrogen Receptors Aandbin Paratesticular Tissues in Boys Operated On For Unilateral Cryptorchidism Between The 1 and 4 Years of LifeDocument5 pagesExpression of Estrogen Receptors Aandbin Paratesticular Tissues in Boys Operated On For Unilateral Cryptorchidism Between The 1 and 4 Years of LifeHamdan Yuwafi NaimNo ratings yet
- Elevated Rates of Testosterone-Related Disorders in Women With Autism Spectrum ConditionsDocument8 pagesElevated Rates of Testosterone-Related Disorders in Women With Autism Spectrum ConditionsaleelrosNo ratings yet
- ArticuloDocument7 pagesArticuloDulceEspinozaLNo ratings yet
- Association Between Male Genital Anomalies and Adult Male Reproductive Disorders A Population-Based Data Linkage Study Spanning More Than 40 YearsDocument8 pagesAssociation Between Male Genital Anomalies and Adult Male Reproductive Disorders A Population-Based Data Linkage Study Spanning More Than 40 YearsMade Moniaga PrawiraNo ratings yet
- Lab Genetics 1Document10 pagesLab Genetics 1Nurul Iman Che AwangNo ratings yet
- Ref 3Document12 pagesRef 3Tiago BaraNo ratings yet
- A Case Study About Klinefelter SyndromeDocument7 pagesA Case Study About Klinefelter SyndromehoyNo ratings yet
- Puberty Suppression Medicine or MalpracticeDocument35 pagesPuberty Suppression Medicine or Malpracticebashomatsuo50% (2)
- Ambiguous Genitalia: Comparative Role of Pelvic Ultrasonography and GenitographyDocument6 pagesAmbiguous Genitalia: Comparative Role of Pelvic Ultrasonography and GenitographyEni Maria SiscaNo ratings yet
- Consensus Statement On Management of Intersex DisordersDocument15 pagesConsensus Statement On Management of Intersex DisordersBarbara G. PiresNo ratings yet
- Sex Redefined - Revista NatureDocument4 pagesSex Redefined - Revista NatureWilliam Harris100% (1)
- Pericentric Inversion of Chromosome 1 and 9 in A Case With Recurrent Miscarriage in EgyptDocument3 pagesPericentric Inversion of Chromosome 1 and 9 in A Case With Recurrent Miscarriage in EgypthandikaNo ratings yet
- Achondroplasia and PregnancyDocument4 pagesAchondroplasia and PregnancyCristina GalloNo ratings yet
- Diagnosing Congenital Malformations in The FetusDocument34 pagesDiagnosing Congenital Malformations in The FetusMonica SurduNo ratings yet
- Study of Incidence of Congenital Anomalies in New Borns: Dr. Kanan Shah, Dr. C.A.PensiDocument3 pagesStudy of Incidence of Congenital Anomalies in New Borns: Dr. Kanan Shah, Dr. C.A.PensiDayuKurnia DewantiNo ratings yet
- Genetic Counseling in TranslocationsDocument15 pagesGenetic Counseling in TranslocationsAsma HMILANo ratings yet
- Preliminary Evidence That Prenatal Alcohol Damage May Be Visible in - 2005 - AlcDocument10 pagesPreliminary Evidence That Prenatal Alcohol Damage May Be Visible in - 2005 - Alcabrigoderoca2No ratings yet
- 17 PDFDocument6 pages17 PDFGinsha Audia KusumoNo ratings yet
- Klinefelter Syndrome ExplainedDocument2 pagesKlinefelter Syndrome ExplainedAica PamintuanNo ratings yet
- Limb Mammary Syndrome: A New Genetic Disorder With Mammary Hypoplasia, Ectrodactyly, and Other Hand/Foot Anomalies Maps To Human Chromosome 3q27Document9 pagesLimb Mammary Syndrome: A New Genetic Disorder With Mammary Hypoplasia, Ectrodactyly, and Other Hand/Foot Anomalies Maps To Human Chromosome 3q27Jane LiuNo ratings yet
- Multi-Disciplinary Study of Smith-Magenis SyndromeDocument8 pagesMulti-Disciplinary Study of Smith-Magenis SyndromeAraNo ratings yet
- Fertility issues in disorders of sex developmentDocument15 pagesFertility issues in disorders of sex developmentEletícia SousaNo ratings yet
- Klinefelter Early DiagnosedDocument7 pagesKlinefelter Early DiagnosedPratita Jati PermatasariNo ratings yet
- Letter To The Editor: Midline Field Defects and Hirschsprung DiseaseDocument2 pagesLetter To The Editor: Midline Field Defects and Hirschsprung DiseaseAraNo ratings yet
- X Chromosome: Genetics Home ReferenceDocument10 pagesX Chromosome: Genetics Home ReferenceAditya SelvarajanNo ratings yet
- Genetic Diagnosis of Short Stature AdvancesDocument12 pagesGenetic Diagnosis of Short Stature Advancesfidyaangraeni 61No ratings yet
- Isochromosome Paper-CorrectionDocument6 pagesIsochromosome Paper-CorrectionponnambalamNo ratings yet
- Childhood and Adolescence Voyages in Development 5th Edition Rathus Solutions ManualDocument36 pagesChildhood and Adolescence Voyages in Development 5th Edition Rathus Solutions Manualaudiblycaribbeeuwiq100% (11)
- Childhood Voyages in Development 5th Edition Rathus Solutions ManualDocument15 pagesChildhood Voyages in Development 5th Edition Rathus Solutions ManualJenniferAguilarrfiax100% (12)
- Emj 43 2 166 169Document4 pagesEmj 43 2 166 169Nisarga GowdaNo ratings yet
- Autismo EstudioDocument41 pagesAutismo Estudiomauricio lopezNo ratings yet
- Cytogenetic Analysis of Male InfertilityDocument7 pagesCytogenetic Analysis of Male InfertilityIOSRjournal100% (1)
- Study of Molecular Cytogenetic Analysis To Determine The Genetic Defect of A PatientDocument6 pagesStudy of Molecular Cytogenetic Analysis To Determine The Genetic Defect of A PatientInternational Journal of Innovative Science and Research Technology100% (1)
- Reviewer Ni VinaceDocument7 pagesReviewer Ni VinaceVinace OmandamNo ratings yet
- An Example of The Utility of Genomic Analysis For Fast and Accurate Clinical Diagnosis of Complex Rare PhenotypesDocument8 pagesAn Example of The Utility of Genomic Analysis For Fast and Accurate Clinical Diagnosis of Complex Rare PhenotypesGlauce L TrevisanNo ratings yet
- Infant Gender Selection & Personalized Medicine: Consumer's GuideFrom EverandInfant Gender Selection & Personalized Medicine: Consumer's GuideNo ratings yet
- 12-11-2022-1668238142-6-Impact - Ijrbm-01.Ijrbm Smartphone Features That Affect Buying Preferences of StudentsDocument7 pages12-11-2022-1668238142-6-Impact - Ijrbm-01.Ijrbm Smartphone Features That Affect Buying Preferences of StudentsImpact JournalsNo ratings yet
- 14-11-2022-1668421406-6-Impact - Ijrhal-01. Ijrhal. A Study On Socio-Economic Status of Paliyar Tribes of Valagiri Village AtkodaikanalDocument13 pages14-11-2022-1668421406-6-Impact - Ijrhal-01. Ijrhal. A Study On Socio-Economic Status of Paliyar Tribes of Valagiri Village AtkodaikanalImpact JournalsNo ratings yet
- 15-10-2022-1665806338-6-IMPACT - IJRBM-1. IJRBM Theoretical and Methodological Problems of Extra-Budgetary Accounting in Educational InstitutionsDocument10 pages15-10-2022-1665806338-6-IMPACT - IJRBM-1. IJRBM Theoretical and Methodological Problems of Extra-Budgetary Accounting in Educational InstitutionsImpact JournalsNo ratings yet
- 19-11-2022-1668837986-6-Impact - Ijrhal-2. Ijrhal-Topic Vocational Interests of Secondary School StudentsDocument4 pages19-11-2022-1668837986-6-Impact - Ijrhal-2. Ijrhal-Topic Vocational Interests of Secondary School StudentsImpact JournalsNo ratings yet
- 19-11-2022-1668838190-6-Impact - Ijrhal-3. Ijrhal-A Study of Emotional Maturity of Primary School StudentsDocument6 pages19-11-2022-1668838190-6-Impact - Ijrhal-3. Ijrhal-A Study of Emotional Maturity of Primary School StudentsImpact JournalsNo ratings yet
- 09-12-2022-1670567289-6-Impact - Ijrhal-06Document17 pages09-12-2022-1670567289-6-Impact - Ijrhal-06Impact JournalsNo ratings yet
- 09-12-2022-1670567569-6-Impact - Ijrhal-05Document16 pages09-12-2022-1670567569-6-Impact - Ijrhal-05Impact JournalsNo ratings yet
- Effect of Sahaja Yoga Meditation in Reducing Anxiety Level of Class Vi Students Towards English As A Second LanguageDocument8 pagesEffect of Sahaja Yoga Meditation in Reducing Anxiety Level of Class Vi Students Towards English As A Second LanguageImpact JournalsNo ratings yet
- 27-10-2022-1666851544-6-IMPACT - IJRANSS-2. IJRANSS - A Review On Role of Ethics in Modern-Day Research Assignment - 1Document6 pages27-10-2022-1666851544-6-IMPACT - IJRANSS-2. IJRANSS - A Review On Role of Ethics in Modern-Day Research Assignment - 1Impact JournalsNo ratings yet
- 11-10-2022-1665489521-6-IMPACT - IJRHAL-Analysing The Matrix in Social Fiction and Its Relevance in Literature.Document6 pages11-10-2022-1665489521-6-IMPACT - IJRHAL-Analysing The Matrix in Social Fiction and Its Relevance in Literature.Impact JournalsNo ratings yet
- 21-09-2022-1663757720-6-Impact - Ijranss-3. Ijranss - The Role and Objectives of Criminal LawDocument8 pages21-09-2022-1663757720-6-Impact - Ijranss-3. Ijranss - The Role and Objectives of Criminal LawImpact JournalsNo ratings yet
- Influence of Erotic Nollywood Films Among Undergraduates of Lead City University, Ibadan, NigeriaDocument12 pagesInfluence of Erotic Nollywood Films Among Undergraduates of Lead City University, Ibadan, NigeriaImpact JournalsNo ratings yet
- 28-10-2022-1666956219-6-Impact - Ijrbm-3. Ijrbm - Examining Attitude ...... - 1Document10 pages28-10-2022-1666956219-6-Impact - Ijrbm-3. Ijrbm - Examining Attitude ...... - 1Impact JournalsNo ratings yet
- 12-10-2022-1665566934-6-IMPACT - IJRHAL-2. Ideal Building Design y Creating Micro ClimateDocument10 pages12-10-2022-1665566934-6-IMPACT - IJRHAL-2. Ideal Building Design y Creating Micro ClimateImpact JournalsNo ratings yet
- 05-09-2022-1662375638-6-Impact - Ijranss-1. Ijranss - Analysis of Impact of Covid-19 On Religious Tourism Destinations of Odisha, IndiaDocument12 pages05-09-2022-1662375638-6-Impact - Ijranss-1. Ijranss - Analysis of Impact of Covid-19 On Religious Tourism Destinations of Odisha, IndiaImpact JournalsNo ratings yet
- 21-09-2022-1663757902-6-Impact - Ijranss-4. Ijranss - Surgery, Its Definition and TypesDocument10 pages21-09-2022-1663757902-6-Impact - Ijranss-4. Ijranss - Surgery, Its Definition and TypesImpact JournalsNo ratings yet
- 25-10-2022-1666681548-6-IMPACT - IJRHAL-4. IJRHAL-Challenges of Teaching Moral and Ethical Values in An Age of Instant GratificationDocument4 pages25-10-2022-1666681548-6-IMPACT - IJRHAL-4. IJRHAL-Challenges of Teaching Moral and Ethical Values in An Age of Instant GratificationImpact JournalsNo ratings yet
- 07-09-2022-1662545503-6-Impact - Ijranss-2. Ijranss - Role of Bio-Fertilizers in Vegetable Crop Production A ReviewDocument6 pages07-09-2022-1662545503-6-Impact - Ijranss-2. Ijranss - Role of Bio-Fertilizers in Vegetable Crop Production A ReviewImpact JournalsNo ratings yet
- 02-09-2022-1662112193-6-Impact - Ijrhal-1. Ijrhal - Shifting Gender Roles A Comparative Study of The Victorian Versus The Contemporary TimesDocument12 pages02-09-2022-1662112193-6-Impact - Ijrhal-1. Ijrhal - Shifting Gender Roles A Comparative Study of The Victorian Versus The Contemporary TimesImpact JournalsNo ratings yet
- 22-09-2022-1663824012-6-Impact - Ijranss-5. Ijranss - Periodontics Diseases Types, Symptoms, and Its CausesDocument10 pages22-09-2022-1663824012-6-Impact - Ijranss-5. Ijranss - Periodontics Diseases Types, Symptoms, and Its CausesImpact JournalsNo ratings yet
- 24-09-2022-1664015374-6-Impact - Ijranss-6. Ijranss - Patterns of Change Among The Jatsas Gleaned From Arabic and Persian SourcesDocument6 pages24-09-2022-1664015374-6-Impact - Ijranss-6. Ijranss - Patterns of Change Among The Jatsas Gleaned From Arabic and Persian SourcesImpact JournalsNo ratings yet
- 20-09-2022-1663649149-6-Impact - Ijrhal-2. Ijrhal - A Review of Storytelling's Role and Effect On Language Acquisition in English Language ClassroomsDocument10 pages20-09-2022-1663649149-6-Impact - Ijrhal-2. Ijrhal - A Review of Storytelling's Role and Effect On Language Acquisition in English Language ClassroomsImpact JournalsNo ratings yet
- 28-09-2022-1664362344-6-Impact - Ijrhal-4. Ijrhal - Understanding The Concept of Smart City and Its Socio-Economic BarriersDocument8 pages28-09-2022-1664362344-6-Impact - Ijrhal-4. Ijrhal - Understanding The Concept of Smart City and Its Socio-Economic BarriersImpact JournalsNo ratings yet
- 01-10-2022-1664607817-6-Impact - Ijrbm-2. Ijrbm - Innovative Technology in Indian Banking Sector-A Prospective AnalysisDocument4 pages01-10-2022-1664607817-6-Impact - Ijrbm-2. Ijrbm - Innovative Technology in Indian Banking Sector-A Prospective AnalysisImpact JournalsNo ratings yet
- Comparison of Soil Properties Collected From Nalgonda, Ranga Reddy, Hyderabad and Checking Its Suitability For ConstructionDocument8 pagesComparison of Soil Properties Collected From Nalgonda, Ranga Reddy, Hyderabad and Checking Its Suitability For ConstructionImpact JournalsNo ratings yet
- Effect of Organizational Commitment On Research and Development Performance of Academics: An Empirical Analysis in Higher Educational InstitutionsDocument12 pagesEffect of Organizational Commitment On Research and Development Performance of Academics: An Empirical Analysis in Higher Educational InstitutionsImpact JournalsNo ratings yet
- 19-09-2022-1663587287-6-Impact - Ijrhal-3. Ijrhal - Instability of Mother-Son Relationship in Charles Dickens' Novel David CopperfieldDocument12 pages19-09-2022-1663587287-6-Impact - Ijrhal-3. Ijrhal - Instability of Mother-Son Relationship in Charles Dickens' Novel David CopperfieldImpact JournalsNo ratings yet
- 29-08-2022-1661768824-6-Impact - Ijrhal-9. Ijrhal - Here The Sky Is Blue Echoes of European Art Movements in Vernacular Poet Jibanananda DasDocument8 pages29-08-2022-1661768824-6-Impact - Ijrhal-9. Ijrhal - Here The Sky Is Blue Echoes of European Art Movements in Vernacular Poet Jibanananda DasImpact JournalsNo ratings yet
- Study and Investigation On The Red and Intangible Cultural Sites in Guangdong - Chasing The Red Mark and Looking For The Intangible Cultural HeritageDocument14 pagesStudy and Investigation On The Red and Intangible Cultural Sites in Guangdong - Chasing The Red Mark and Looking For The Intangible Cultural HeritageImpact JournalsNo ratings yet
- 25-08-2022-1661426015-6-Impact - Ijrhal-8. Ijrhal - Study of Physico-Chemical Properties of Terna Dam Water Reservoir Dist. Osmanabad M.S. - IndiaDocument6 pages25-08-2022-1661426015-6-Impact - Ijrhal-8. Ijrhal - Study of Physico-Chemical Properties of Terna Dam Water Reservoir Dist. Osmanabad M.S. - IndiaImpact JournalsNo ratings yet
- Monoclonal Antibodies: K. Prameela Department of Biotechnology Gitam UniversityDocument20 pagesMonoclonal Antibodies: K. Prameela Department of Biotechnology Gitam Universityanjanakaveri100% (1)
- Functions of Liver in Human BodyDocument3 pagesFunctions of Liver in Human BodyalikhanbalouchNo ratings yet
- Chapter 16 Homework Part IIDocument6 pagesChapter 16 Homework Part IIKvn4N6No ratings yet
- SBI recruitment for probationary officersDocument16 pagesSBI recruitment for probationary officersRahul PambharNo ratings yet
- Modified SYLLABUS PDFDocument9 pagesModified SYLLABUS PDFSHRIKANTNo ratings yet
- Domains & Kingdoms of LifeDocument14 pagesDomains & Kingdoms of LifeRam Iyer100% (1)
- Histology of The TissuesDocument31 pagesHistology of The TissuesAbiola NerdNo ratings yet
- Introduction To Eumetazoa: The True Animals'Document22 pagesIntroduction To Eumetazoa: The True Animals'jeanette8riosNo ratings yet
- Agilent Bioanalyzer Application CompediumDocument104 pagesAgilent Bioanalyzer Application CompediumShi Jie Pang100% (1)
- ARDSDocument6 pagesARDSarcobaleno589No ratings yet
- PHB Production in Azomonas, Acinteobacter and Bacillus Species: Isolation, Screening and IdentificationDocument8 pagesPHB Production in Azomonas, Acinteobacter and Bacillus Species: Isolation, Screening and IdentificationInternational Medical PublisherNo ratings yet
- Scientific-Benefits-Of-Meditation-Pdf-Liveanddare ComDocument14 pagesScientific-Benefits-Of-Meditation-Pdf-Liveanddare Comapi-321697736No ratings yet
- Domain Study Healthcare AnalyticsDocument3 pagesDomain Study Healthcare AnalyticsAzeem KhaliphaNo ratings yet
- Managing Severe Asthma Attacks in ChildrenDocument8 pagesManaging Severe Asthma Attacks in ChildrenIrani VianzaNo ratings yet
- GS Gene Linker Uv Chamber PDFDocument19 pagesGS Gene Linker Uv Chamber PDFPatricia MendozaNo ratings yet
- Antidiarrheal DrugsDocument7 pagesAntidiarrheal Drugsmwaithira71682No ratings yet
- Health: Minidoka County Joint School District #331Document13 pagesHealth: Minidoka County Joint School District #331Minidoka County Joint School DistrictNo ratings yet
- Approach To MyopathyDocument22 pagesApproach To MyopathySurat Tanprawate100% (2)
- HepatitisDocument46 pagesHepatitisGusti Tirtha Drag JrNo ratings yet
- Canonum de Ius Virtus Naturae PDFDocument216 pagesCanonum de Ius Virtus Naturae PDFsimon martin ryderNo ratings yet
- ESMO Checklist Breast Cancer Patient Related Treatment WorkflowDocument1 pageESMO Checklist Breast Cancer Patient Related Treatment WorkflowsameeramwNo ratings yet
- Community EssayDocument9 pagesCommunity Essayolylmqaeg100% (2)
- Antisense Drug TechnologyDocument12 pagesAntisense Drug TechnologyARAFAT MIAHNo ratings yet
- Slide Review CriteriaDocument1 pageSlide Review CriteriaanggaririnNo ratings yet
- The Guide - A.G. - B.V. - 31-10-'13Document282 pagesThe Guide - A.G. - B.V. - 31-10-'13reginaldocastelaNo ratings yet
- A2LA - Policy On Estimating Measurement Uncertainity For Life Sciences Testing LabsDocument10 pagesA2LA - Policy On Estimating Measurement Uncertainity For Life Sciences Testing Labszahids2kNo ratings yet
- HiperbillirubinemiaDocument7 pagesHiperbillirubinemiaBrenda RomeroNo ratings yet