You might also like
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Androgenetic AlopeciaDocument22 pagesAndrogenetic AlopeciaYuliannisa Nyunyun100% (1)
- 13 Hair Boosting Remedies 2Document35 pages13 Hair Boosting Remedies 2Anonymous 2P5vzcSoDNo ratings yet
- Vitamin Water - Arnel Ricafranca PDFDocument32 pagesVitamin Water - Arnel Ricafranca PDFAlaa EssamNo ratings yet
- 88 Hair Growth DisordrDocument24 pages88 Hair Growth DisordrAlivia Soeraya100% (1)
- Insurance Fraud PPT (Final)Document30 pagesInsurance Fraud PPT (Final)Gaurav Savlani83% (6)
- Alopecia: Mrs. Neeraja Rajiv Asst Professor Cardio-RespDocument52 pagesAlopecia: Mrs. Neeraja Rajiv Asst Professor Cardio-RespNEERAJA O S O S100% (1)
- Cairo: Pilbeam's Mechanical Ventilation, 6th EditionDocument7 pagesCairo: Pilbeam's Mechanical Ventilation, 6th EditionLesly Peinado Torres100% (1)
- Estudio XL HAIR - Alopecia AreataDocument32 pagesEstudio XL HAIR - Alopecia AreataIrina KucevichuteNo ratings yet
- Control System 1Document34 pagesControl System 1Shrinivas Prabhu100% (4)
- Control System 1Document34 pagesControl System 1Shrinivas Prabhu100% (4)
- Dr. Salma Samir: Lecturer of Dermatology & Aesthetic Medicine Alex. Faculty of MedicineDocument38 pagesDr. Salma Samir: Lecturer of Dermatology & Aesthetic Medicine Alex. Faculty of MedicineSamir Omar0% (1)
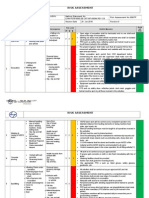
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- MCQS Computer Terminology Practice QuestionsDocument129 pagesMCQS Computer Terminology Practice QuestionsCalvin GreenNo ratings yet
- Hair Loss in WomenDocument11 pagesHair Loss in WomenLENINNo ratings yet
- Immediate DenturesDocument35 pagesImmediate DenturesSimran SahniNo ratings yet
- Hair Loss in Women Book: How any Woman Can Put an End To Hair Loss and Fast-track Hair RecoveringFrom EverandHair Loss in Women Book: How any Woman Can Put an End To Hair Loss and Fast-track Hair RecoveringNo ratings yet
- Hair Loss In Women: The Ultimate Hair Loss Book For Every WomanFrom EverandHair Loss In Women: The Ultimate Hair Loss Book For Every WomanNo ratings yet
- Professional Growth and DevelopmentDocument154 pagesProfessional Growth and DevelopmentNina Anne Paracad100% (3)
- Annexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistDocument5 pagesAnnexure I: Block / Building Fire Safety Audit-Check List Fire Safety Audit ChecklistGaurav Singh67% (3)
- Androgenic Alopecia Finished ThesisDocument73 pagesAndrogenic Alopecia Finished ThesisAkshay R Aiyar100% (2)
- HRM Case StudyDocument21 pagesHRM Case StudyNabil Eyg Iakini100% (1)
- SSIPDocument4 pagesSSIPGlenn Clemente100% (2)
- Alopecia Areata PresentationDocument12 pagesAlopecia Areata Presentationpcjoy2100% (1)
- Comprehensive Overview and Treatment Update On Hair LossDocument8 pagesComprehensive Overview and Treatment Update On Hair LossmirafitrNo ratings yet
- Alopecia AreataDocument4 pagesAlopecia AreataMellisa Aslamia AslimNo ratings yet
- Comprehensive Overview and Treatment Update On Hair LossDocument9 pagesComprehensive Overview and Treatment Update On Hair LossZuldan KaramiNo ratings yet
- Guidelines for Managing Alopecia AreataDocument8 pagesGuidelines for Managing Alopecia AreataPedro López CastroNo ratings yet
- Hairloss Cream002Document5 pagesHairloss Cream002JaTi NurwigatiNo ratings yet
- Anzai 2020Document6 pagesAnzai 2020Belen Llanquilef NavarroNo ratings yet
- Tsunemi 2016Document8 pagesTsunemi 2016Nicolas BaronNo ratings yet
- Hairrestoration Intheethnicpatient Andreviewofhair Transplant FundamentalsDocument8 pagesHairrestoration Intheethnicpatient Andreviewofhair Transplant FundamentalsGabriel Urrea BoteroNo ratings yet
- Efficacy of Low Level Laser Therapy in The Treatment of Alopecia AreataDocument6 pagesEfficacy of Low Level Laser Therapy in The Treatment of Alopecia AreataRo KohnNo ratings yet
- Alopecia Areata ManejoDocument14 pagesAlopecia Areata ManejoVar AndaNo ratings yet
- Alpha-Gf GFC Study International Journal of Research in DermatologyDocument10 pagesAlpha-Gf GFC Study International Journal of Research in DermatologyraoNo ratings yet
- Alopecia Androgenetica 2009Document9 pagesAlopecia Androgenetica 2009Franklin ArandaNo ratings yet
- AlopeciaDocument12 pagesAlopeciasonamNo ratings yet
- HAIRLOSSDocument16 pagesHAIRLOSSIrawan Pandu Buditomo100% (1)
- Bio 3Document42 pagesBio 3manojkumar200624No ratings yet
- Androgenetic Alopecia and Current Methods of TreatmentDocument4 pagesAndrogenetic Alopecia and Current Methods of TreatmentPamela TrujilloNo ratings yet
- Superior Dutasteride Treatment for AlopeciaDocument83 pagesSuperior Dutasteride Treatment for AlopeciadumpalacaNo ratings yet
- AutoimmuneDocument5 pagesAutoimmuneTiara ArazsyNo ratings yet
- PDIA Art 28497-10Document6 pagesPDIA Art 28497-10Arturo OteroNo ratings yet
- Valproate-Induced Hair Loss - What To Tell Patients - MDedge PsychiatryDocument3 pagesValproate-Induced Hair Loss - What To Tell Patients - MDedge Psychiatrydo leeNo ratings yet
- AlopeciaDocument11 pagesAlopeciaAnonymous kltUTa100% (1)
- Hair and Scalp Evaluation: The Trichogram: Practical DermatologyDocument10 pagesHair and Scalp Evaluation: The Trichogram: Practical DermatologyFelipe NunesNo ratings yet
- An Approach To Patients With AlopeciaDocument12 pagesAn Approach To Patients With AlopeciaMariana de la VegaNo ratings yet
- Alopecia HandoutDocument4 pagesAlopecia HandoutEmAlNourNo ratings yet
- Effect of Micro Organisms On Food Quality and SafetyDocument15 pagesEffect of Micro Organisms On Food Quality and Safetyohiomahmaria995No ratings yet
- PriceNEJMrev PrimaryDocument10 pagesPriceNEJMrev PrimarySunilSainiNo ratings yet
- Hair Loss and Its Management in ChildrenDocument23 pagesHair Loss and Its Management in ChildrenDiana Sofia GonzalezNo ratings yet
- Evaluation of Hair Loss Among Young Females of Age Group (18-25) YearsDocument3 pagesEvaluation of Hair Loss Among Young Females of Age Group (18-25) YearsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Half ResultDocument45 pagesHalf Resultmanojkumar200624No ratings yet
- Hair Restoration Update: by DR - Tarek Ahmed Said Lecturer of Plastic Surgery, Cairo UniversityDocument27 pagesHair Restoration Update: by DR - Tarek Ahmed Said Lecturer of Plastic Surgery, Cairo UniversityHamid Reza TeymouriNo ratings yet
- TOP Dermatologic Therapy - 2021 - Piccolo - Trichobiolight A New Effective Protocol in The Treatment of Androgenetic AlopeciaDocument8 pagesTOP Dermatologic Therapy - 2021 - Piccolo - Trichobiolight A New Effective Protocol in The Treatment of Androgenetic Alopeciaandre.ramosNo ratings yet
- Reading Part A Hair LossDocument6 pagesReading Part A Hair Lossfernanda1rondelliNo ratings yet
- Contents DetDocument4 pagesContents DetNhật Nguyễn QuangNo ratings yet
- Nanoparticle Based Herbal Remedies for Alopecia ManagementDocument17 pagesNanoparticle Based Herbal Remedies for Alopecia ManagementVikas JhawatNo ratings yet
- Everett2020 Recent Advances in The Treatment of Trichotillomania - Hair Pulling DisorderDocument37 pagesEverett2020 Recent Advances in The Treatment of Trichotillomania - Hair Pulling DisorderRoberto CarvalhoNo ratings yet
- Female Pattern Hair LossDocument5 pagesFemale Pattern Hair LossDavid Fernando Rojas BayonaNo ratings yet
- Medicina Estetica M8T8Document9 pagesMedicina Estetica M8T8Rawal Chemical ComplexNo ratings yet
- Celavost I TerapijaDocument3 pagesCelavost I Terapijasantasa99No ratings yet
- Microneedling en Alopecia Androgenética Comparando Dos Profundidades Diferentes de MicroagujasDocument7 pagesMicroneedling en Alopecia Androgenética Comparando Dos Profundidades Diferentes de MicroagujasLuisa BucioNo ratings yet
- Physical Means of Treating Unwanted Hair: R W & T S. ADocument10 pagesPhysical Means of Treating Unwanted Hair: R W & T S. Adipika awindaNo ratings yet
- Amer 2021Document8 pagesAmer 2021Dâmaris LaignierNo ratings yet
- Hair Loss and Herbs For TreatmentDocument13 pagesHair Loss and Herbs For TreatmentmuhtevaNo ratings yet
- Hair Loss and Herbs For Treatment Lourith2013Document13 pagesHair Loss and Herbs For Treatment Lourith2013leonardorodriguezsabateNo ratings yet
- 6 Be 46595156Document5 pages6 Be 46595156Ikhwan AmirudinNo ratings yet
- Hair Fall Causes and TreatmentDocument18 pagesHair Fall Causes and TreatmentJo CanensNo ratings yet
- Xu2017 PDFDocument13 pagesXu2017 PDFalysa ahadyahNo ratings yet
- Xu 2017Document13 pagesXu 2017Stella SunurNo ratings yet
- Uk Capability: I C C C - P PDocument9 pagesUk Capability: I C C C - P PShrinivas PrabhuNo ratings yet
- Seating ArrangementDocument1 pageSeating ArrangementShrinivas PrabhuNo ratings yet
- Sangam Vartha IV IssueDocument8 pagesSangam Vartha IV IssueShrinivas PrabhuNo ratings yet
- Project Report: Vocational Training atDocument32 pagesProject Report: Vocational Training atShrinivas PrabhuNo ratings yet
- Chapter 2Document82 pagesChapter 2Kavitha Selvaraj50% (2)
- Manipal BTech Phys Course Plan 2014janDocument4 pagesManipal BTech Phys Course Plan 2014janShrinivas PrabhuNo ratings yet
- Sangam Vartha IV IssueDocument8 pagesSangam Vartha IV IssueShrinivas PrabhuNo ratings yet
- Stepper Motor OperationDocument6 pagesStepper Motor OperationPavan KumarNo ratings yet
- Atomic Physics Modified-RPDocument73 pagesAtomic Physics Modified-RPShrinivas PrabhuNo ratings yet
- A Technical Guide To Stepper MotorsDocument6 pagesA Technical Guide To Stepper MotorsShrinivas PrabhuNo ratings yet
- Diffraction Modified Aug2011Document93 pagesDiffraction Modified Aug2011Shrinivas PrabhuNo ratings yet
- MM Soil 280311Document217 pagesMM Soil 280311AnandKuttiyanNo ratings yet
- Step Motor BasicsDocument2 pagesStep Motor BasicsShrinivas PrabhuNo ratings yet
- Stepper Motor OperationDocument6 pagesStepper Motor OperationPavan KumarNo ratings yet
- General Category-Fee Circular For Ay 2013-14Document1 pageGeneral Category-Fee Circular For Ay 2013-14Shrinivas PrabhuNo ratings yet
- Step Motor BasicsDocument2 pagesStep Motor BasicsShrinivas PrabhuNo ratings yet
- 7 SegmentasDocument7 pages7 SegmentasShrinivas PrabhuNo ratings yet
- Case Studies Based On NI HardwareDocument29 pagesCase Studies Based On NI HardwareShrinivas PrabhuNo ratings yet
- Project #5 Even and Odd Signals: S S L U M (© 2 0 0 1, M H - A)Document3 pagesProject #5 Even and Odd Signals: S S L U M (© 2 0 0 1, M H - A)Shrinivas PrabhuNo ratings yet
- Laplace Circuit AnalysisDocument25 pagesLaplace Circuit AnalysisLighto LastoNo ratings yet
- 2 DiffractdionDocument124 pages2 DiffractdionShrinivas PrabhuNo ratings yet
- General Category-Fee Circular For Ay 2013-14Document1 pageGeneral Category-Fee Circular For Ay 2013-14Shrinivas PrabhuNo ratings yet
- Read MeDocument1 pageRead MeShrinivas PrabhuNo ratings yet
- MartiniDocument3 pagesMartinivitubioluNo ratings yet
- Understanding patients' and healthcare providers' confidentiality rights and obligationsDocument2 pagesUnderstanding patients' and healthcare providers' confidentiality rights and obligationsMelody B. MiguelNo ratings yet
- A Comparative Study of The Efficacy of Cedarwood Oil, Coconut Oil and Dish Wash Liquid As Alternatives To Xylene As Deparaffinizing AgentsDocument98 pagesA Comparative Study of The Efficacy of Cedarwood Oil, Coconut Oil and Dish Wash Liquid As Alternatives To Xylene As Deparaffinizing AgentszzzzNo ratings yet
- Couchiching FN Toll BoothDocument8 pagesCouchiching FN Toll BoothpegspirateNo ratings yet
- Central Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFDocument398 pagesCentral Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFRomeo-Remus RaffaiNo ratings yet
- Nursing Care Plans for Respiratory and Circulatory IssuesDocument5 pagesNursing Care Plans for Respiratory and Circulatory IssuesApryll Kristin Villaluna ZafeNo ratings yet
- Measurement and Correlates of Family Caregiver Self-Efficacy For Managing DementiaDocument9 pagesMeasurement and Correlates of Family Caregiver Self-Efficacy For Managing DementiariskhawatiNo ratings yet
- BSBMKG502 Task 2Document9 pagesBSBMKG502 Task 2Diana PulidoNo ratings yet
- A Study To Assess The Effectiveness of Hydrabadi Mix Ball On Nutritional Status Among Malnourished Under Five Year Children at Selected Anganwadi in Barabanki, Uttar PradeshDocument15 pagesA Study To Assess The Effectiveness of Hydrabadi Mix Ball On Nutritional Status Among Malnourished Under Five Year Children at Selected Anganwadi in Barabanki, Uttar PradeshEditor IJTSRDNo ratings yet
- UKHO Survey Specification Acoustic V3 Jul18Document102 pagesUKHO Survey Specification Acoustic V3 Jul18Iqbal FauzanNo ratings yet
- Child Abuse Research JournalDocument9 pagesChild Abuse Research JournaladrianekattnerNo ratings yet
- Vacation With Sunny Leone - Without FlightDocument4 pagesVacation With Sunny Leone - Without FlightkalidasdoraemonNo ratings yet
- Petroleum Gases, Liquefied Petroleum Gas: IdentificationDocument4 pagesPetroleum Gases, Liquefied Petroleum Gas: IdentificationdigecaNo ratings yet
- Managing STEM AthletesDocument13 pagesManaging STEM Athletesanon_629662799No ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAlintana JobelleNo ratings yet
- The Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LDocument8 pagesThe Effect of Potassium Permanganate (KMnO4) Concentration and Storage Time on Quality of California Papaya (Carica papaya LSyifa UlNo ratings yet
- Human Resources Manager in San Jose CA Resume Priscilla CramerDocument2 pagesHuman Resources Manager in San Jose CA Resume Priscilla CramerPriscillaCramerNo ratings yet
- CPT 2021 guide for identifying medical proceduresDocument7 pagesCPT 2021 guide for identifying medical proceduresChester FernandezNo ratings yet
- Otto Chemie PVT LTD: Material Safety Data SheetDocument4 pagesOtto Chemie PVT LTD: Material Safety Data Sheetenes duhanNo ratings yet
- Nurs 5019 - Soap Note 41-60 Year OldDocument7 pagesNurs 5019 - Soap Note 41-60 Year Oldapi-308904543100% (1)
- PDF Biaya MaternityDocument2 pagesPDF Biaya MaternityKurnia Yuliyanti RahayuNo ratings yet
- Giraffe and Panda Warmer TRM M1128921 Rev PDocument230 pagesGiraffe and Panda Warmer TRM M1128921 Rev PRonnelSerranoNo ratings yet