You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Code of Ethics Short Version-EnGDocument2 pagesCode of Ethics Short Version-EnGpurpleanvilNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- PDFDocument10 pagesPDFpurpleanvilNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- APMA Position StatementDocument3 pagesAPMA Position StatementpurpleanvilNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- RANZCOG Letter AustraliaDocument2 pagesRANZCOG Letter AustraliapurpleanvilNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- SA Doula Brochure Aug08Document2 pagesSA Doula Brochure Aug08purpleanvil100% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Beyond The Breech Trial. Maggie BanksDocument4 pagesBeyond The Breech Trial. Maggie Bankspurpleanvil100% (2)
- Term Breech Trial CommentaryDocument3 pagesTerm Breech Trial CommentarypurpleanvilNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Midirs Waterbirth ProfDocument8 pagesMidirs Waterbirth Profpurpleanvil100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Good Birth Guide South Australia: Brought To You byDocument4 pagesThe Good Birth Guide South Australia: Brought To You bypurpleanvilNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- NMC Circular 8 2006 29 MarchDocument4 pagesNMC Circular 8 2006 29 Marchpurpleanvil100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Test QuestionsDocument4 pagesTest QuestionsRoel AczonNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Pregnancy (Y)Document64 pagesPregnancy (Y)Mohamed AbbasNo ratings yet
- Alison P He Ngeka PresentationsDocument19 pagesAlison P He Ngeka PresentationsAlisonNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Pengaruh Pijat Oksitosin Terhadap Produksi AsipadaibupostpartumDocument4 pagesPengaruh Pijat Oksitosin Terhadap Produksi AsipadaibupostpartumSilfa RianyNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Shree Siddaganga Institute of Nursing Sciences and Research CentreDocument8 pagesShree Siddaganga Institute of Nursing Sciences and Research CentreSanthosh.S.UNo ratings yet
- Chapter 11: Operative Obstetrics by SiaDocument2 pagesChapter 11: Operative Obstetrics by Siakristel ludangcoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Normal Labour& Abnormal LabourDocument23 pagesNormal Labour& Abnormal LabourThetnaungsoe100% (1)
- Conduct of Normal Vaginal Delivery ProcedureDocument10 pagesConduct of Normal Vaginal Delivery ProcedureAshish GuptaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Fourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric NursingDocument35 pagesFourth Year B SC Nursing Obstetric and Gynaecological Nursing Obstetric Nursingsandeepv080% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Severe Birth Asphyxia: Risk Factors As Seen in A Tertiary Institution in The Niger Delta Area of NigeriaDocument9 pagesSevere Birth Asphyxia: Risk Factors As Seen in A Tertiary Institution in The Niger Delta Area of NigeriaSteven JonesNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Cattle Breeding GuideDocument30 pagesCattle Breeding GuideLintangNo ratings yet
- Jurnal Rupture Perineum 3Document6 pagesJurnal Rupture Perineum 3Muh AqwilNo ratings yet
- Contraction Ring, Uterine Rupture, Precipitate LaborDocument4 pagesContraction Ring, Uterine Rupture, Precipitate LaborJessica Carmela CasugaNo ratings yet
- Pasien SC Bulan Januari 2019: Tanggal MasukDocument25 pagesPasien SC Bulan Januari 2019: Tanggal MasukMaria AmabiNo ratings yet
- Post Partum GymnasticDocument5 pagesPost Partum GymnasticDewi UtariNo ratings yet
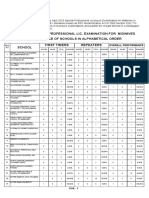
- April 2023 Special Professional Lic. Examination For MidwivesDocument2 pagesApril 2023 Special Professional Lic. Examination For MidwivesRapplerNo ratings yet
- WaterbirthDocument2 pagesWaterbirthapi-405873549No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Maternity Services Escalation Policy 5.1Document29 pagesMaternity Services Escalation Policy 5.1Bader NammurNo ratings yet
- Animal ReproductionDocument93 pagesAnimal ReproductionunattractiveyouNo ratings yet
- Manejo RCIU Basado en EstadíosDocument5 pagesManejo RCIU Basado en EstadíosRodrigoEscobedoNo ratings yet
- Antenatal Perineal MassageDocument2 pagesAntenatal Perineal MassageFarid NurdiansyahNo ratings yet
- ECPM 2021 European Congress of Perinatal MedicineDocument1 pageECPM 2021 European Congress of Perinatal MedicineAl DiNo ratings yet
- Kehamilan GandaDocument18 pagesKehamilan GandaLaris Donar Marukkap SihombingNo ratings yet
- GRADE 4 WEEK 4 and 5Document7 pagesGRADE 4 WEEK 4 and 5jommel vargasNo ratings yet
- OBSTETRICS Enhancement - FINAL COPY 1Document17 pagesOBSTETRICS Enhancement - FINAL COPY 1Jan Joseph BanzuelaNo ratings yet
- Persistent Inaccuracies in Completion of Medical Certificates of Stillbirth: A Cross-Sectional StudyDocument8 pagesPersistent Inaccuracies in Completion of Medical Certificates of Stillbirth: A Cross-Sectional StudyPhilip BeardNo ratings yet
- 3Document6 pages3Yuuki Chitose (tai-kun)No ratings yet
- Assisted Breech Delivery1Document28 pagesAssisted Breech Delivery1swatisinghnigeria100% (4)
- Expectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameDocument3 pagesExpectant Mother'S and Baby Information Sheet: Given Name: Middle Name: Last NameLeslie D. Aton86% (14)
- Lesson Plan On PROM and PLDocument11 pagesLesson Plan On PROM and PLArjun NeupaneNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)