You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- HHS Public Access: The Nature of Immune Responses To Urinary Tract InfectionsDocument20 pagesHHS Public Access: The Nature of Immune Responses To Urinary Tract InfectionsElena CuibanNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 1 s2.0 S2589537021005216 MainDocument13 pages1 s2.0 S2589537021005216 MainElena CuibanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Tandogdu 2016Document6 pagesTandogdu 2016Elena CuibanNo ratings yet
- Clostridioides Difficile Infection in Patients WitDocument10 pagesClostridioides Difficile Infection in Patients WitElena Cuiban100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Mihaescu 2021Document19 pagesMihaescu 2021Elena CuibanNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Gkha 2019Document172 pagesGkha 2019Elena CuibanNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Embolizare Splenica PartialaDocument5 pagesEmbolizare Splenica PartialaElena CuibanNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Thrombocytopenia in Chronic Liver Disease: Lessons From Transplanted PatientsDocument5 pagesThrombocytopenia in Chronic Liver Disease: Lessons From Transplanted PatientsElena CuibanNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Established and New-Generation Antithrombotic Drugs in Patients With Cirrhosis - Possibilities and CaveatsDocument9 pagesEstablished and New-Generation Antithrombotic Drugs in Patients With Cirrhosis - Possibilities and CaveatsElena CuibanNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- P394 WindActions PDFDocument32 pagesP394 WindActions PDFzhiyiseowNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Recall, Initiative and ReferendumDocument37 pagesRecall, Initiative and ReferendumPhaura Reinz100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- CA Inter Group 1 Book November 2021Document251 pagesCA Inter Group 1 Book November 2021VISHAL100% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Profile On Sheep and Goat FarmDocument14 pagesProfile On Sheep and Goat FarmFikirie MogesNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Fake PDFDocument2 pagesFake PDFJessicaNo ratings yet
- SCDT0315 PDFDocument80 pagesSCDT0315 PDFGCMediaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cdi 2 Traffic Management and Accident InvestigationDocument22 pagesCdi 2 Traffic Management and Accident InvestigationCasanaan Romer BryleNo ratings yet
- Expense Tracking - How Do I Spend My MoneyDocument2 pagesExpense Tracking - How Do I Spend My MoneyRenata SánchezNo ratings yet
- Office Storage GuideDocument7 pagesOffice Storage Guidebob bobNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Gardner Denver PZ-11revF3Document66 pagesGardner Denver PZ-11revF3Luciano GarridoNo ratings yet
- Interruptions - 02.03.2023Document2 pagesInterruptions - 02.03.2023Jeff JeffNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Rating SheetDocument3 pagesRating SheetShirwin OliverioNo ratings yet
- MORIGINADocument7 pagesMORIGINAatishNo ratings yet
- Feasibility Study of Diethyl Sulfate ProductionDocument3 pagesFeasibility Study of Diethyl Sulfate ProductionIntratec SolutionsNo ratings yet
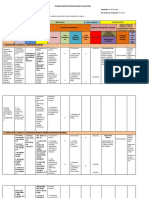
- Fidp ResearchDocument3 pagesFidp ResearchIn SanityNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Cabling and Connection System PDFDocument16 pagesCabling and Connection System PDFLyndryl ProvidoNo ratings yet
- 06-Apache SparkDocument75 pages06-Apache SparkTarike ZewudeNo ratings yet
- Activity Description Predecessor Time (Days) Activity Description Predecessor ADocument4 pagesActivity Description Predecessor Time (Days) Activity Description Predecessor AAlvin LuisaNo ratings yet
- Perkins 20 Kva (404D-22G)Document2 pagesPerkins 20 Kva (404D-22G)RavaelNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Epidemiologi DialipidemiaDocument5 pagesEpidemiologi DialipidemianurfitrizuhurhurNo ratings yet
- Schmidt Family Sales Flyer English HighDocument6 pagesSchmidt Family Sales Flyer English HighmdeenkNo ratings yet
- Basic of An Electrical Control PanelDocument16 pagesBasic of An Electrical Control PanelJim Erol Bancoro100% (2)
- The Internal Environment: Resources, Capabilities, Competencies, and Competitive AdvantageDocument5 pagesThe Internal Environment: Resources, Capabilities, Competencies, and Competitive AdvantageHenny ZahranyNo ratings yet
- Agricultural Economics 1916Document932 pagesAgricultural Economics 1916OceanNo ratings yet
- Reflections On Free MarketDocument394 pagesReflections On Free MarketGRK MurtyNo ratings yet
- CI Principles of EconomicsDocument833 pagesCI Principles of EconomicsJamieNo ratings yet
- Guide For Overseas Applicants IRELAND PDFDocument29 pagesGuide For Overseas Applicants IRELAND PDFJasonLeeNo ratings yet
- Professional Regula/on Commission: Clarita C. Maaño, M.DDocument31 pagesProfessional Regula/on Commission: Clarita C. Maaño, M.Dmiguel triggartNo ratings yet
- 48 Volt Battery ChargerDocument5 pages48 Volt Battery ChargerpradeeepgargNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ARUP Project UpdateDocument5 pagesARUP Project UpdateMark Erwin SalduaNo ratings yet