Professional Documents
Culture Documents
Nrendo 2014 60
Nrendo 2014 60
Uploaded by
Alejandro PvOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Nrendo 2014 60
Nrendo 2014 60
Uploaded by
Alejandro PvCopyright:
Available Formats
NATURE REVIEWS | ENDOCRINOLOGY ADVANCE ONLINE PUBLICATION | 1
Department of
Pediatrics, University of
Groningen, University
Medical Center
Groningen,
Hanzeplein1, 9700RB
Groningen, Netherlands
(F.K., V.W.B., A.K.G.).
Correspondence to:
F.K.
f.kuipers@umcg.nl
Beyond intestinal soapbile acids
in metabolic control
Folkert Kuipers, Vincent W. Bloks and Albert K. Groen
Abstract | Over the past decade, it has become apparent that bile acids are involved in a host of activities
beyond their classic functions in bile formation and fat absorption. The identification of the farnesoid X
receptor (FXR) as a nuclear receptor directly activated by bile acids and the discovery that bile acids are
also ligands for the membrane-bound, G-protein coupled bile acid receptor1 (also known as TGR5) have
opened new avenues of research. Both FXR and TGR5 regulate various elements of glucose, lipid and
energymetabolism. Consequently, a picture has emerged of bile acids acting as modulators of (postprandial)
metabolism. Therefore, strategies that interfere with either bile acid metabolism or signalling cascades
mediated by bile acids may represent novel therapeutic approaches for metabolic diseases. Synthetic
modulators of FXR have been designed and tested, primarily in animal models. Furthermore, the use of bile
acid sequestrants to reduce plasma cholesterol levels has unexpected benefits. For example, treatment of
patients with type2 diabetes mellitus (T2DM) with sequestrants causes substantial reductions in plasma
levels of glucose and HbA
1c
. ThisReview aims to provide an overview of the molecular mechanisms by which
bile acids modulate glucose and energy metabolism, particularly focusing on the glucose-lowering actions
ofbile acid sequestrants in insulin resistant states and T2DM.
Kuipers, F. etal. Nat. Rev. Endocrinol. advance online publication 13 May 2014; doi:10.1038/nrendo.2014.60
Introduction
Bile acids are amphipathic steroids that are synthesized
from cholesterol exclusively in the liver. Bile acids and
bile-acid-like molecules are present in mam mals
and in nonmammalian species, such as fish and nema-
tode worms. The immediate products of the biosyn-
thetic pathways that convert water-insoluble cholesterol
into water-soluble molecules with detergent proper-
ties are referred to as primary bile acids (Figure1).
These molecules are conjugated to either taurine (2-
aminoethanesulphonic acid) or glycine to increase
hydrophilicity, secreted into the bile and then dis char-
ged into the intestine. The chemical diversity of the bile
acid pool present in the body is increased by conver-
sion of primary bile acids into secondary bile acids by
intestinal bacteria (Figure1). Efficient active absorption
of primary bile acids in the terminal ileum and pas sive
absorption of secondary bile acids from the colon, fol-
lowed by hepatic uptake from the portal blood and
resecre tion into bile, results in the accumulation of a
pool of bile acids within the body.
This bile acid pool cycles between the liver and the
intestine (enterohepatic circulation) with a frequency
that is partially determined by the pattern of food
intake. The existence of such a circulating pool ensures
the presence of adequate bile acid concentrations (inthe
millimolar range) at sites of physiological actions;
namely, in the bile canaliculi to promote bile formation,
in the gallbladder to prevent cholesterol crystallization
and in the intestinal lumen to facilitate the absorption
of dietary fat and fat-soluble vitamins.
1
For example, a
bile acid pool with an average size of ~2 g that cycles
~10times each day requires that the liver and intestine
can transport ~20 g of bile acids every 24 h.
2
Highly effec-
tive hepatic and intestinal transport systems have evolved
to ac commodate this flux.
The individual components of the bile acid transport
machinery, which comprise transporter proteins for
uptake and excretion localized at the basolateral and
apical membrane domains of hepatocytes and entero-
cytes (Figure2), have been identified.
35
Defects in these
components have been implicated in human herit-
able diseases with severe phenotypes, such as progres-
sive familial intrahepatic cholestasis (PFIC) types13.
Approximately 5% of the bile acids escape intestinal
reabsorption and are lost in the faeces. This loss of
~0.6 g per day in humans is accurately compensated
for by denovo bile acid synthesis in the liver to main-
tain the pool size and represents a major determinant
of cholesterol turnover.
6
The detergent properties of bile
acids are determined by the number and orientation of
the hydroxyl groups and the presence or absence of an
amino acid moiety (Figure1) and are crucial for bio-
logical functions.
35,7,8
However, these properties might
also impose a risk to cells exposed to high concentrations
Competing interests
F.K. declares that part of the original research referred to in this
article was supported by TiPharma (T1-106) and that he received
an unrestricted research grant from Daiichi Sankyo to evaluate
the effects of colesevelam on bile acid metabolism in humans
and animals. V.W.B. and A.K.G. declare no competing interests.
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
2 | ADVANCE ONLINE PUBLICATION www.nature.com/nrendo
of bile acids. For example, bile acids can cause inflam-
mation, apoptosis and liver cell necrosis. Consequently,
protective mechanisms aimed at lowering intracellular
bile acid concentrations, such as downregulation of
cellular uptake systems and upregulation of detoxify-
ing biotransformation reactions, become active during
accumulation of bile acids. A method for sensing bile
acids is, therefore, required to ensure both the initiation
of mechanisms to protect cells and tight regulation of the
size of the bile acid pool.
The discovery in 1999 that bile acids act as natural
ligands for the transcription factor farnesoid X receptor
(FXR; also known as bile acid receptor or nuclear recep-
tor subfamily1 groupH member4) provided a mecha-
nistic framework for bile acid sensing.
911
The expression
of many genes that encode proteins involved in bile
acid synthesis, transport and metabolism is directly
controlled by bile acids through activation of FXR.
5,12
Furthermore, bile acids were found to serve specific,
hormone-like functions in the control of glucose, lipid
and energy metabolism. The activation of FXR by bile
acids modulates the expression of key metabolic genes;
bile acids also influence metabolism through signal-
ling via the membrane-bound, G-protein coupled bile
acid receptor1 (also known as TGR5). Bile acids can be
considered as metabolic integrators that are particularly
active postprandially. This role could have additional
dimensions through interactions between indi vidual
bile acids and the microbiome, which is another impor-
tant factor in the maintenance of health.
1315
The micro-
biome plays a part in controlling the composition of
the bile acid pool through deconjugation and dehy-
droxylation reactions, and hence also modulates bile
acid signalling functions.
1618
Conversely, bile acids can
inhibit bacterial growth and so influence the compo-
sition of the microbiome.
19
Altered bile acid signalling
might contribute to the development and/or worsen-
ing of components of the metabolic syndrome (hepatic
steato sis, low-grade inflammation, hypertriglyceridae-
mia, low levels of HDL cholesterol or hyperglycaemia).
20
Conse quently, interference with bile acid metabolism or
with bile acid signalling cascades could represent novel
t reatment options.
Key points
Bile acids are amphipathic steroids derived from cholesterol that serve
important physiological functions such as bile formation and intestinal fat
absorption that are dependent on their detergent nature
The discovery of farnesoid X receptor (FXR) and G-protein coupled bile acid
receptor1 (TGR5) as bile acid receptors that regulate glucose, lipid and energy
metabolism has highlighted bile acids as key players in metabolic control
Modulators of bile acid receptors have been developed as potential treatments
for cholestatic liver diseases and metabolic diseases; organ-specific and/or
gene-cluster-selective modulators are expected in the near future
Type2 diabetes mellitus (T2DM) is accompanied by a shift in primary bile acid
synthesis towards cholic acid and a corresponding increase in the secondary
bile acid deoxycholic acid
Beneficial effects of bile acid sequestrants on glucose metabolism in patients
with T2DM could reflect changed compartmentalization of the bile acid pool
that modifies intestinal bile acid signalling
This Review aims to provide a condensed overview
of the modes of action by which bile acids can modu-
late glucose and energy metabolism, particularly focus-
ing on clinically relevant aspects such as the benefi cial
metabolic effects of bariatric surgery and the glucose-
lowering effects of bile acid sequestrants in type 2
di abetes mellitus (T2DM).
Bile acids modulate metabolism
Signal transduction pathways
As shown in Figure2, bile acids have key roles in signal
transduction pathways that involve FXR, fibroblast
growth factor19 (FGF19) and TGR5. Once activated by
bile acids, FXR promotes the release of circulating FGF19
from the ileum, which contributes to the regulation of
hepatic bile acid synthesis and gallbladder function,
21
as well as postprandial energy metabolism.
2224
In addi-
tion, an FXR-independent mode of bile acid signalling
has been identified.
25,26
This pathway involves bile-acid-
induced activation of TGR5.
27,28
Specific roles for bile-
acid mediated TGR5 signalling in the control of energy
and glucose metabolism (for example, promotion of
glucagon-like peptide1 [GLP-1] release by intestinal
Lcells) and in the regulation of enterohepatic circula-
tion dynamics (for example, gallbladder function and
intestinal motility) have been identified.
2732
FXR
FXR is a member of the nuclear receptor superfamily of
transcription factors that comprises 48 family members
in humans.
33
Activation by its ligand causes FXR to form
a heterodimeric complex with another nuclear receptor
family member, retinoic X receptor (RXR), and bind
to specific DNA elements within the promoter regions
of target genes. Once bound to DNA, activated FXR
recruits transcriptional co-regulators and the RNA poly-
merase machinery to initiate gene transcription.
34,35
As
shown in Figure2, SHP, which encodes the SHP protein
(small heterodimer partner, also known as nuclear
receptor subfamily0 groupB member2) is a key target
gene of FXR. Indeed, most of the suppressive effects of
FXR on genes encoding components of the bile acid
synthesis cascade, as well as genes involved in metabo-
lism, are predominantly mediated through activation of
SHP.
3639
Notably, the SHP protein lacks a DNA-binding
domain and functions as a transcriptional repressor by
binding directly to a number of nuclear receptors such as
liver receptor homolog1 (LRH-1, also known as nuclear
receptor subfamily5 groupA member2) to control
expression of cholesterol 7-hydroxylase (also known
as cholesterol 7-monooxygenase or CYP7A1; Figure2).
Expression of the FXR protein is high in organs
that constitute the enterohepatic circulation (liver and
intes tine), but it is also present in white adipose tissue,
kidney, adrenal gland, stomach, pancreas, endothe-
lial cells, vascular smooth muscle cells and cells of the
immune system.
4047
This distribution pattern indicates
a broad spectrum of biological functions that seems to
potentially involve cell types that lack high concentra-
tions of bile acids (for example, adipocytes). Yet, one
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | ENDOCRINOLOGY ADVANCE ONLINE PUBLICATION | 3
of the most intriguing phenotypic characteristics of
whole-body FXR-deficient mice is the presence of small,
in sulin-resistant adipocytes.
42
This phenotype is prob-
ably attributable to a role of FXR in the process of adipo-
cyte differentiation.
44,48
FXR deficiency also prevents
weight gain and the development of hyperglycaemia in
both the leptin-deficient ob/ob mouse model and in lean
C57BL/6N mice during ageing.
4952
Two features of FXR biology require specific atten-
tion in the context of this Review. First, not all bile
acids are equally effective in the activation of FXR. The
ranking of bile acids in this respect is, from the highest
to the lowest potency: chenodeoxycholic acid, deoxy-
cholic acid, lithocholic acid and cholic acid;
9,10
the very
hydrophilic (rodent-specific) bile acid -muricholic
acid might actually exert antagonistic effects.
17,53
Mouse
studies have demonstrated the metabolic consequences
of selective changes in bile acid composition.
18,54,55
For
instance, Haeusler etal. noted that a relative deficiency
of 12-hydroxylated bile acids (cholic and deoxycholic
acids) in mice contributes to a diabetic lipid pheno-
type through impaired FXR signalling.
54
This obser-
vation implies that changes in the composition of the
bile acid pool that might occur in disease states, such as
T2DM (discussed later), or as a consequence of dietary
changes,
56
can influence bile acid signalling in the body.
Likewise, the dynamics of the enterohepatic circulation,
as determined by gallbladder emptying or intestinal
motility, is another relevant parameter that is influenced
by disease and diet.
57
Second, the expression and activity of FXR are modu-
lated by metabolic status. The mRNA levels of FXR are
markedly reduced in the livers of rodent models of type1
diabetes mellitus and T2DM, whereas FXR gene expres-
sion in hepatocytes is modulated by glucose, possibly
via intermediates of the pentose phosphate pathway.
58
Another mode of FXR dysregulation that can occur in
metabolic disease is post-translational modification of
the protein.
34
Thus, phosphorylation of FXR by protein
kinaseC promotes its transcriptional activity.
59
The activ-
ity of FXR is also regulated by glucose fluxes in hepato-
cytes through direct O-GlcNAcylation catalysed by the
hexosamine biosynthetic pathway, which increases FXR
protein stability and transcriptional activity.
60
Finally,
FXR is a target of the NAD-dependent protein deacety-
lase sirtuin-1 that removes acetyl groups from modified
lysine residues in histones and transcription factors.
61
Acetylation increases FXR stability but inhibits its ability
to heterodimerize with RXR, bind DNA and induce gene
expression. In two well-established models of obesity and
insulin resistance (ob/ob mice and mice fed a high-fat
diet), elevated levels of acetylated FXR were detected in
the liver, a situation that could be reversed by treatment
with the sirtuin-1 activator resveratrol.
61
FGF19
A number of the physiological effects of bile acids are
now known to be mediated by FGF19 (or its counterpart
FGF15 in mice and rats). Expression of FGF19 is almost
exclusively restricted to the terminal ileum, which
corres ponds to the site where bile acids are actively taken
up by the ileal sodium/bile acid cotransporter (ASBT;
Figure2). Bile acids induce ileal expression of the FGF19
gene through FXR.
62
In addition, fat-soluble vitaminsA
and D regulate FGF15 gene expression in mice via the
vitaminD3 receptor (VDR) and retinoid-responsive
nuclear receptors.
63
Diet1 was identified as another
modulator of FGF15 production. The Diet1 protein is
expressed in enterocytes of the small intestine and muta-
tions in its gene confer resistance to hyper lipidaemia
Primary
bile acids
Secondary
bile acids
Cholesterol
Cholic acid
Taurocholic acid
HO
HO OH
OH
OH
O
HO OH
OH
NH
O
S
OH
O O
MDCA
3,6OH
HDCA
3,6OH
UDCA
3,7OH
HCA
3,6,7OH
MCA
3,6,7OH
LCA
3OH
DCA
3,12OH
Intestine
Liver
Cholesterol
(5-cholesten-3-ol)
CA
3,7,12OH
CDCA
3,7OH
MCA
3,6,7OH
MCA
3,6,7OH
Figure 1 | Schematic overview of primary and secondary bile acid species. The
conversion of cholesterol into bile acids in the liver involves multiple enzymatic
steps.
137,138
The initial products of this cascade are the primary bile acids (CA and
CDCA in humans and CA, MCA and MCA in rodents). Primary bile acids are
conjugated to either taurine or glycine, secreted into the bile and stored in the
gallbladder to be discharged into the intestinal lumen upon ingestion of a meal.
Thechemical diversity of the pool of bile acids is enhanced by the actions of
intestinal bacteria to form secondary bile acids (DCA and LCA in humans).
Abbreviations: MCA, -muricholic acid (3,6,7-trihydroxy-5-cholanoic acid);
MCA, -muricholic acid (3,6,7-trihydroxy-5-cholanoic acid); MCA, -muricholic
acid (3,6,7-trihydroxy-5-cholanoic acid); CA, cholic acid (3,7,12-trihydroxy-
5-cholanoic acid); CDCA, chenodeoxycholic acid (3,7-dihydroxy-5-cholanoic acid);
DCA, deoxycholic acid (3,12-dihydroxy-5-cholanoic acid); HCA, hyocholic
acid (3,6,7-trihydroxy-5-cholanoic acid); HDCA, hyodeoxycholic acid (3,6-
dihydroxy-5-cholanoic acid); LCA, lithocholic acid (3-hydroxy-5-cholanoic acid);
MDCA, murideoxycholic acid (3,6-dihydroxy-5-cholanoic acid); UDCA,
ursodeoxycholic acid (3,7-dihydroxy-5-cholanoic acid).
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
4 | ADVANCE ONLINE PUBLICATION www.nature.com/nrendo
and atherosclerosis in mice, which suggests that FGF15/
FGF19 action constitutes an important control point in
the relationship between bile acid metabolism and lipid
homeostasis.
64
FGF19 is excreted from the enterocytes
into the portal circulation by an unknown route and
travels to the liver, where it exerts pleiotropic effects on
hepatic bile acid, lipid and glucose metabolism. These
effects require binding of FGF19 to FGF receptor4
(FGFR4), which is localized at the plasma membrane of
the hepatocytes. Interaction of FGFR4 with the acces-
sory protein -klotho is necessary to activate signal ling
through an incompletely elucidated signal transduc tion
path way, probably involving SHP to suppress CYP7A1,
the rate-controlling enzyme in bile acid synthe sis
(Figure2).
62,65,66
Indeed, a postprandial rise in plasma
levels of FGF19 precedes a reduction in the plasma levels
of C4, a marker of hepatic bile acid synthesis, which
highlights a potential causal relationship.
67
The role of the FXRFGF15 axis in the control of
bile acid synthesis was confirmed in numerous rodent
studies.
68,69
Nonetheless, the contributions of direct
(FXR) and indirect (FGF15) control remain unclear, as
does the level of coordination between these factors.
70
Unexpectedly, FGF15-deficient mice are glucose
intolerant and store less glycogen in their livers than do
wild-type mice, whereas intravenous administration of
FGF19 to overnight fasted wild-type mice stimulates
hepatic glycogen synthesis.
23
Supplementation with
FGF19 induces phosphorylation and inactivation of
the and subunits of glycogen synthase kinase, which
in turn leads to increased hepatic glycogen synthesis
and increased glucose disposal. This effect is insulin-
independent, which might explain why mice with defec-
tive insulin signalling retain the ability to store glycogen
in their livers.
71
Thus, increased ileal bile acid signalling
induces an insulin-like effect with respect to glycaemic
control but does not promote lipogenesis owing to the
involvement of different signal transduction pathways.
21
Of note, reduced plasma levels of FGF19 have been
reported among patients with T2DM.
72,73
TGR5
The TGR5 receptor is highly expressed in liver cells other
than hepatocytes, including Kupffer cells and cholangio-
cytes, and also in gallbladder epithelial cells and immune
cells.
30
In addition, TGR5 is expressed in brown adipose
tissue, the enteric nervous system, the central nervous
system, muscle and in the small intestinal and colonic
enteroendocrine Lcells that produce GLP-1 (Figure2).
31
Activation of TGR5 by bile acids, or by other endogenous
ligands or synthetic agonists,
74,75
triggers internalization
of the receptor, increased intra cellular levels of cAMP
and activation of protein kinaseA, which in turn leads
to increased phosphorylation of target proteins. The
consequences of TGR5 activation are cell-type-specific
and comprise anti-inflammatory effects, gallbladder
relaxation, increased intestinal motility, increased energy
expenditure in brown adipose tissue and improved
glucose metabolism and insulin sensitivity.
The addition of cholic acid to a high-fat diet resulted
in elevated plasma levels of bile acids that attenu-
ated diet-induced obesity and insulin resistance in
mice.
76
Activation of TGR5 in brown adipose tissue by
elevated circulating bile acid levels was postulated to
increase energy expenditure through activation of the
type2 iodothyronine deiodinase that, in turn, leads
to increased levels of active T
4
and induction of genes
involved in energy metabolism. These effects were
absent in mice fed normal chow and the identity of the
per missive factor associated with intake of the high-fat
diet has remained elusive. Suppression of bile acid syn-
thesis and reduction of the bile acid pool using the FXR
agonist GW4064 was associated with reduced energy
expenditure, pronounced weight gain and glucose intol-
erance in mice fed a high-fat diet.
77
Counter-intuitively,
treatment with the bile acid sequestrant colestimide
improved metabolic control in mice fed a high-fat diet
through stimulation of energy expenditure, a change that
Hepatocyte
Enterocyte
L-cell
FGFR4
-Klotho
BA
GLP-1
FGF15/19
OST/ ASBT
BA
resin
BA
BA
BA
resin
VDR
Diet1
FXR BA
LXR
FXR
BA
SHP
HNF4A Cholesterol
PXR CYP7A1
SHP
TGR5
NTCP Metabolic effects BA
Metabolic effects
Metabolic effects
FGF15/19
BA
GLP-1
FGF15/19
ABCB11
Figure 2 | Schematic overview of bile acid signalling within the enterohepatic
circulation. Bile acids are actively secreted from hepatocytes into the bile
canaliculi by the ATP-dependent transporter ABCB11. Most bile acids are
reabsorbed in the terminal ileum via ASBT. Within ileal enterocytes, bile acids
stimulate production of FGF19 (FGF15 in mice). Upon reaching the liver, FGF19
activates signalling pathways that repress bile acid synthesis. The presence of a
resin (sequestrant) in the intestinal lumen prevents ileal bile acid uptake and
FGF19 production. Bile acids in the portal circulation are taken up by the liver via
NTCP for re-secretion into bile. As hepatic extraction is not complete, part of the
intestine-derived bile acids spill over to the systemic circulation to act on
peripheral organs and tissues via FXR-initiated or TGR5-initiated signalling
pathways. Bile acids present in the lower gastrointestinal tract (unbound and
sequestrant-bound) are able to activate TGR5 on Lcells to promote production
and secretion of GLP-1. Abbreviation: BA, bile acid.
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | ENDOCRINOLOGY ADVANCE ONLINE PUBLICATION | 5
coincided with activation of thermogenesis in brown
adipose tissue.
78
A role for TGR5 in energy homeostasis is further
supported by observations that female (but not male)
TGR5-deficient mice become more obese than wild-
type controls when fed a high-fat diet.
79
Further more,
treatment with a TGR5 agonist reduces the develop-
ment of obesity in wild-type mice under the same diet-
ary conditions.
80
Analysis of TGR5 expression in human
pe rthyroid adipose tissue biopsy samples (obtained
dur ing thyroid surgery) showed that TGR5 expression
was positive ly correlated to the resting metabolic rate.
81
Bariatric surgery and metabolic control
Insights into the metabolic actions of bile acids have
sparked interest in their potential role in (patho)physio-
logy, for instance in mediating the beneficial effects of
bariatric surgery, which has become an important thera-
peutic option for morbid obesity. Evidence is accumu-
lating that the metabolic improvements that occur as a
result of the various surgical procedures available are
not merely caused by mechanical restriction of meal
size or malabsorption of macronutrients. A putative
link to human energy metabolism was provided by a
study that found plasma bile acid levels to be appreci-
ably higher among patients with obesity after bariatric
surgery than in weight-matched control individuals,
suggesting that bile acids could contribute to improved
metabolic control after weight-loss surgery.
82
Nonethe-
less, a study that compared the metabolic consequences
of two bariatric procedures to reduce morbid obesity
reported that gastric bypass resulted in elevated fasting
and post prandial levels of bile acids and increased TGR5
si gnalling when compared with gastric banding.
83
The increased levels of bile acids associated with gas-
tric bypass did not, however, predict changes in glu-
cose homeostasis or energy metabolism. Steinert etal.
com pared time-dependent effects of gastric bypass and
sleeve gastrectomy in patients with morbid obe s ity.
84
Pre surgery levels of plasma bile acids were lower in
patients with obesity than in a cohort of healthy indi-
vi duals. In both patient groups, marked increases in
GLP-1 levels and improved glycaemic control were evi-
dent at 1week and 3months after surgery. Yet, fasting
and postprandial levels of bile acids were appreciably
elevated only at 1year after surgery, suggesting that an
increased pool of circulating bile acids was not causal
in this respect. In support of these findings, Brufau
etal.
85
compared hypermetabolic patients (indi viduals
in whom energy expenditure is high relative to body
surface) with liver cirrhosis and elevated plasma bile
acid levels to control individuals matched for sex, age
and BMI and found that neither total nor individual
plasma bile acid levels corre lated with energy expendi-
ture. However, another study that compared small
groups of patients with a lcohol-induced cirrhosis of
the liver and healthy individuals did find a positive
relationship between fasting plasma bile acid levels
and energy metabolism.
86
Clearly, the relevance of ele-
vated levels of circulating bile acids in the control of
energy metabolism after bariatric surgery remains to
be fullyestablished.
Conversely, some data indicate that altered bile acid
kin etics owing to the surgically induced anatomical
changes within the enterohepatic c irculationparticu-
larly upon Roux-en-Y gastric bypass surgerymight
be of physiological relevance. Indeed, statistically sig-
nificantly elevated plasma FGF19 levels have been
reported in patients with obesity after gastric bypass
surgery,
8789
which is indicative of enhanced bile acid
signalling in the terminal ileum. Elevated levels of
FGF19 might improve the metabolic status of patients
through effects on carbo hydrate metabolism in the liver
and white adipose tissue (reviewed elsewhere
90
). In addi-
tion, increased FGF19 levels could also act in the brain
to induce insulin- independent plasma glucose lower-
ing.
91
Likewise, enhanced intestinal bile acid signalling
through TGR5, owing to the presence of elevated bile
acid concentrations in the distal part of the intestinal
tract, might be involved.
27,28,31
In this scenario, excess bile
acids present in the intestinal lumen activate TGR5 asso-
ciated with Lcells, which leads to secretion of GLP-1 into
the circulation to improve intestinal motility, as well as
hepatic and pancreatic function to reduce insulin resist-
ance.
92
Indeed, gastric bypass surgery is associated with
a dramatic increase in the secretion of GLP-1 (as well as
other gut hormones, such as peptideYY).
93
The observed
changes in the levels of gut hormones might contrib-
ute to a sustained improvement of glucose metabolism
under such conditions.
94
Targeting bile acid metabolism
Given the new insights into bile acid functions discussed
here, strategies for treatment of metabolic disease and
cholestatic liver disease have been defined and tested in
model systems and in selected patient groups (reviewed
elsewhere
27,95102
).
Bile acids
Bile acids have been used for decades in the treatment
of gallstones (chenodeoxycholic acid and ursodeoxy-
cholic acid), cholestatic liver diseases (ursodeoxycholic
acid) and genetic conditions that affect bile acid synth-
esis (cholic acid and chenodeoxycholic acid). Data on
the overall metabolic consequences of such treatments
are few and mainly descriptive in nature.
5
However,
treatment of gallstones with chenodeoxycholic acid has
been reported to reduce not only the levels of plasma
tri glycerides (a positive effect) but also levels of HDL
cholesterol (a potentially negative effect), probably in
part through FXR-mediated modulation of the expres-
sion of target genes, such as APOA1, APOC1, APOC3
and CETP. For bile acids and most of the synthetic
compounds (for example, FXR agonists, discussed
later) tested in animal models, it should be stressed that
beneficial effects were only apparent under conditions
of compromised health status (for example, in mouse
models of genetic or diet-induced obesity and insulin
resistance).
27
Evidently, interference with bile acid sig-
nalling is effective only when the metabolic and signal
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
6 | ADVANCE ONLINE PUBLICATION www.nature.com/nrendo
transduction pathways are balanced at a new set point in
response to a prevailing insulin-resistant, nutrient-rich
state and/or when altered bile acid metabolism perse is
causative in disease development.
FXR agonists
A number of clinical studies have been initiated with syn-
thetic FXR agonists, such as obeticholic acid (6- ethyl-
chenodeoxycholic acid, also known as INT-747), as
potential therapies for T2DM and nonalcoholic steato-
hepatitis.
27,97
For example, a phase 2 double-blind
placebo-controlled proof-of-concept study tested the
effects of obeticholic acid in patients with both T2DM
and nonalcoholic fatty liver disease.
103
Administration of
obeticholic acid (25 mg or 50 mg daily) for 6weeks was
well-tolerated, increased insulin sensitivity and reduced
markers of liver inflammation and fibrosis. Extensive
discussion of these findings is beyond the scope of
thisReview.
Bile acid sequestrants
During the past few years, bile acid sequestration, an old
trick to lower plasma LDL cholesterol levels for preven-
tion of cardiovascular diseases, has showed unexpected
beneficial effects among patients with hyperlipidaemia
and T2DM. These effects may be explained by the role
of bile acids in metabolic control. Interruption of the
entero hepatic circulation of bile acids by either ileal
bypass surgery or administration of bile acid seques-
trants, such as cholestyramine, colestipol and coleseve-
lam, is effective in prevention of coronary heart disease
by lowering LDL cholesterol.
104,105
Withdrawal of bile
acids from the circulation is also associated with slightly
elevated plasma levels of triglycerides and HDL choles-
terol.
20
Bile acid sequestrants in general, and the second-
generation compound colesevelam in particular, also
improve glycaemic control in patients with T2DM.
106113
Administration of colesevelam plus common anti dia-
betic agents such as metformin caused a mean reduc-
tion in fasting blood glucose levels of 0.83 mmol/l
and a drop in mean HbA
1c
level of 0.5%.
114
The original
studies that were the subject of a Cochrane review on
this topic
114
provided the basis for approval of coleseve-
lam by the FDA as an adjunct therapy for glycaemic
control in patients with T2DM in 2008. Data on the
long-term effects of colesevelam on microvascular and
macro vascular complications and cardiovascular risk in
patients with T2DM are still awaited.
Mechanisms of actionclinical insights
The mode of action by which sequestrants improve gly-
caemic control remains to be elucidated. Bile acid seques-
tration might act by reducing the size or changing the
composition of the bile acid pool and/or by al tering
the kinetics of enterohepatic bile acid cycling. One study
addressed this issue by quantitatively assessing bile acid
metabolism in patients with T2DM using state-of-
the-art stable isotope techniques and quantifying the
effects of colesevelam on bile acid metabolism in these
patients.
115
Male participants with T2DM and a group
of control individuals matched for age, sex and BMI
were studied at baseline and after 2weeks and 8weeks
of treatment (Figure3). The patients with T2DM had an
increased cholic acid synthesis rate, an increased input
rate of deoxycholic acid, a correspondingly increased
deoxycholic acid pool size and a trend toward a smaller
chenodeoxycholic acid pool size; however, the total
bile acid pool size was unchanged. A preponderance
of deoxycholic acid among patients with T2DM was
also found in a study that used multiple experimental
methods to detect metabolites in blood samples after
fasting.
116
These data are concordant with those from
previous studies that reported altered bile acid metabo-
lism in patients with T2DM;
117121
however, these earlier
studies were restricted to measures of bile acid compo-
sition alone or total bile acid synthesis without data on
individual bile acid species.
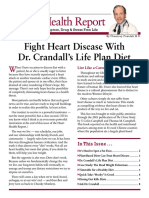
As expected (but never before quantified), the effects
of colesevelam on bile acid metabolism were both pro-
found and specific for the type of bile acid.
115
Treatment
with colesevelam doubled the synthesis of cholic acid in
both the diabetic and control groups, whereas chenode-
oxycholic acid synthesis was stimulated in both groups
to a lesser extent (Figure3). The reduction of fasting and
postprandial levels of FGF19 observed in both groups
upon sequestrant therapy might have contributed to the
differential derepression of bile acid synthesis. The cholic
acid pool size was doubled after treatment in patients
and controls, whereas the chenodeoxycholic acid and
deoxycholic acid pool sizes were statistically significantly
decreased. The differences in individual pool sizes bal-
anced each other so that, unexpectedly, no statistically
significant differences in total bile acid pool size were
T2DM
Baseline Colesevelam
1,769 mol
per day
2,983mol
per day
Bile acid synthesis Bile acid pool size
CA
Baseline Colesevelam
4,706 mol 3,955 mol
2,226mol
per day
4,259mol
per day
4,816mol 4,902 mol
Controls
CDCA DCA
Figure 3 | The effects of T2DM and sequestration on bile acid kinetics. The
synthesis rates (CA, CDCA) and the pool sizes (CA, CDCA, DCA) of the major bile
acid species in humans were quantified by stable isotope dilution techniques in
male individuals with T2DM and control individuals without diabetes mellitus
matched for age, sex and BMI, prior to treatment (baseline) and after 8weeks of
treatment with the bile acid sequestrant colesevelam. Data from Brufau etal.
115
Abbreviations: CA, cholic acid (3,7,12-trihydroxy-5-cholanoic acid); CDCA,
chenodeoxycholic acid (3,7-dihydroxy-5-cholanoic acid); DCA, deoxycholic acid
(3,12-dihydroxy-5-cholanoic acid); T2DM, type2 diabetes mellitus.
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | ENDOCRINOLOGY ADVANCE ONLINE PUBLICATION | 7
induced. As chenodeoxycholic acid and deoxycholic
acid are more hydrophobic than cholic acid, colesevelam
increased the hydrophilicity of the circulating bile acid
pool (which, in theory, led to a decrease in the activity of
bile acids on both FXR and TGR5). Also in this study,
115
treatment with colesevelam reduced insulin resistance
(as determined by HOMA) and fasting glucose and
HbA
1c
levels. However, no relationships between any
of the kinetic parameters of bile acid metabolism and
changes in glucose metabolism or markers of insulin
resistance were found.
A double-blind randomized placebo-controlled study
evaluated a 12-week course of colesevelam therapy in
a group of patients with T2DM who were also being
treated with diet and exercise, sulphonylurea, metformin
or a combination thereof.
122
Stable isotope techniques
were used to quantify relevant parameters of glucose
metabolism invivo. Compared with placebo, treat-
ment with colesevelam improved the following meas-
ures of glycaemic control: plasma glucose levels, HbA
1c
levels, fasting plasma glucose clearance and glycolytic
disposal of oral glucose. However, colesevelam did not
alter gluco neogenesis or the rate at which glucose levels
increased in blood after an oral glucose load, which is
a measure of the rate of intestinal absorption. Fasting
endogenous glucose production and glycogenolysis
both remained unchanged in the colesevelam group
but showed an increase in the group assigned placebo.
Treatment with colesevelam increased total levels of
GLP-1 (in line with previous animal experiments
123
)
and improved -cell function; however, plasma insulin
levels, hepatic glucagon levels and insulin resistance
(as determined by HOMA) remained unchanged.
Consistent with previous findings,
67,115
circulating
levels of FGF19 were found to be reduced after bile acid
sequestration. In another study, the effects of coleseve-
lam on fasting and postprandial glucose metabolism
were evaluated among patients with T2DM who were
receiving monotherapy with metformin.
124
Colesevelam
decreased both fasting and postprandial plasma levels
of glucose and HbA
1c
in the absence of any changes in
the levels of insulin. Surprisingly, postprandial GLP-1
concentrations were not altered by colesevelam in this
study. Endogenous glucose production and glucose dis-
posal remained unchanged; however, the rate at which
meal-derived glucose appeared in the bloodstream
was decreased by colesevelam, which suggests either
increased splanchnic uptake of ingested glucose or
delayed intestinal absorption. The partly differing out-
comes of these two studies of colesevelam
122,124
might
be related to differences in adjuvant therapies and/or in
analytical approaches.
Mechanisms of actionexperimental insights
Animal studies have been performed to compare the
effects of sequestration on the kinetics of bile acids and
glu cose in lean mice versus obese and diabetic (db/db)
mice.
125,126
Administration of colesevelam reduced intestinal bile
acid absorption by 30% and stimulated hepatic bile acid
synthesis (particularly that of cholic acid) by twofold to
threefold both in lean and obese mice.
125
The size of the
circulating bile acid pool was not reduced in response
to colesevelammeaning that increased faecal loss
was accurately compensated for by hepatic synthesis
whereas plasma bile acid levels were lower in treated
mice than in untreated mice.
125
Colesevelam reduced
the levels of plasma glucose and insulin resistance and
increased the metabolic clearance of glucose (by 37%)
in the db/db mice, but did not affect gluconeogenesis
and total hepatic or endogenous glucose production in
either of the mouse strains evaluated. Improved meta-
bolic clearance of glucose in treated db/db mice was
accompanied by normalization of strongly elevated acyl-
carnitine concentrations in muscle and plasma, particu-
larly of the acylcarnitines containing saturated palmitic
acid (C16:0) and stearic acid (C18:0) fatty acid species.
Normalization of these markers of inefficient mitochon-
drial fatty acid oxidation might reflect an improved
capability to switch to the utilisation of glucose.
126
In contrast to the situation described for bariatric
surgery, FGF19 is clearly unlikely to be involved in the
meta bolic improvement observed upon bile acid seques-
trant therapy in humans and mice. Increased release of
GLP-1 from ileal Lcells induced by fatty acids (that reach
the ileum owing to defective micellar solubilization and
impaired absorption) has been proposed to underpin the
mechanism for improved glycaemic control in res ponse
to colesevelam in patients with T2DM.
127
Although this
mechanism probably contributes to the observed effects,
it is now evident that bile acids can induce GLP-1 secre-
tion from the luminal side of the intestinal cells in the
ileum and colon, even when bound to a sequestrant.
27,53,93
Indeed, colonic administration of cholic acid in mice
and healthy humans produces elevated levels of GLP-1 in
the circulation.
128,129
Likewise, mice that lack the ileal bile
acid uptake protein ASBT (Figure2) exhibit improved
glycaemic control when fed a high-fat diet that is asso-
ciated with elevated plasma GLP-1 levels, as do mice
treated with an ASBT inhibitor.
130
Clearly, in both situa-
tions, there is overflow of bile acids into the colon owing
to defective uptake from the ileum.
Induction of intestinal GLP-1 expression by high
levels of sequestrant-bound bile acids and unabsorbed
fatty acids could contribute to the metabolic improve-
ments observed in db/db mice.
125
Intriguingly, high
expression levels of hepatic FGF21 were also found in
these mice in response to colesevelam.
126
Overexpression
of FGF21 in the livers of diabetic rodents improves
glucose clearance owing to the actions of FGF21 on
muscle and adipose tissue.
131133
In the aforementioned studies,
125,126
no quantitative
effects of bile acid sequestration on hepatic glucose
fluxes were found. However, Potthoff etal.
128
reported
that treatment of diet-induced obese mice with coleseve-
lam reduced hepatic glucose production by suppression
of hepatic glycogenolysis. This effect was partly ascribed
to activation of TGR5 and release of GLP-1 because it
could be blocked by a GLP-1 antagonist. Accordingly, the
ability of colesevelam to reduce glycaemia, spare hepatic
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrendo
glycogen and induce secretion of GLP-1 was compro-
mised in TGR5-deficient mice.
128
Thus, although the
influence of bile acid sequestration on glycaemic control
is evident in metabolically compromised humans and
animals, the underlying mechanism(s) seem to vary in
accordance with the prevailing metabolic status.
Future perspectives
The area of bile acid research has become tremendously
active in the past few years. A number of beneficial and
adverse metabolic effects have been linked to interfer-
ence with bile acid homeostasis and signalling mediated
by bile acids. Interestingly, both increased (following
bariatric surgery) and decreased (upon use of seques-
trants) plasma bile acid levels were shown to be associ-
ated with beneficial effects on energy metabolism and
glycaemic control in humans. The exact reason for this
apparent contradiction is not yet clear but may involve
differential effects on the dynamics of enterohepatic
cycling of the different bile acid species by these inter-
ventions. In this respect, more insight into the meta-
bolic actions of the individual bile acid species invivo is
required. From a therapeutic point of view, development
of organ- selective and/or gene-cluster-specific modula-
tors of FXR is warranted. Agonists that selectively target
intestinal FXR may be particularly useful for treatment
of obesity- associated disorders. Lately, the interaction
between intestinal microbiota and bile acid metabolism
has become en vogue and data indicate that, in addition
to the so-called short-chain fatty acids, bile acids may act
as prime signal transducing molecules between micro-
biota and host metabolism.
134
Many of these studies have
been carried out in animal models; it is important to
note that major differences in bile acid metabolism exist
across the animal kingdom that have to be taken into
account when interpreting the results. In the current
Review, we have focused on the interactions of bile acids
with FXR and TGR5 and ignored other nuclear recep-
tors such as pregnaneX receptor, constitutive androstane
receptor and VDR that also interact with certain bile
acid species. The interaction between the various nuclear
receptor networks in determining the overall metabolic
activity of bile acids invivo deserves further attention.
Conclusions
Evidence is accumulating that bile acids play a crucial
but complex part in coordinating the whole-body res-
ponse to ingestion of food. The physiological and chem-
ical properties of bile acids are essential for effective
uptake of dietary fat and fat-soluble vitamins. By activat-
ing signal transduction pathways via the receptors FXR
and TGR5, bile acids also contribute to the integration
of an adequate postprandial response. These pathways
pro vide promising targets for pharmacological interven-
tion in metabolic diseases. However, in view of the com-
plexity of the metabolic networks involved, the dynamic
nature of the enterohepatic circulation and its constitu-
ents, and the fact that signalling pathways mediated by
bile acids can simultaneously exert health- promoting
and adverse effects, a one size fits all approach will not
be successful. Clearly, both pathway-specific and cell-
type- selective interference will be required to ensure
t herapies are effective.
In conclusion, bile acids should not be considered
as merely intestinal soap but rather as integrators and
mod ulators of key metabolic responses. Exposure to high
levels of bile acids in fetal life (for example, in the off-
spring of mothers with cholestasis during preg nancy)
can program susceptibility to metabolic dis ease later
in life.
135,136
These observations underscore the impor-
tant relationship between bile acids and the control
ofmetabolism.
Review criteria
PubMed was searched for relevant topics, using the
search terms bile acids or bile salts in combination
with sequestrants, resins, type2 diabetes,
glycemic control, glucose-lowering mechanisms,
energy metabolism, FXR, TGR5, FGF15, FGF19,
microbiome and metabolic control, without publication
time constraints. References cited in this article include
both original research and reviews by experts in the field.
1. Hofmann, A.F. The enterohepatic circulation
of bile acids in mammals: form and functions.
Front. Biosci. 14, 25842598 (2009).
2. Stellaard, F., Sackmann, M., Sauerbruch, T. &
Paumgartner, G. Simultaneous determination of
cholic acid and chenodeoxycholic acid pool sizes
and fractional turnover rates in human serum
using 13C-labeled bile acids. J.Lipid Res. 25,
13131319 (1984).
3. Meier, P.J. & Stieger, B. Bile salt transporters.
Annu. Rev. Physiol. 64, 635661 (2002).
4. Trauner, M., Wagner, M., Fickert, P. & Zollner, G.
Molecular regulation of hepatobiliary transport
systems: clinical implications for understanding
and treating cholestasis. J.Clin. Gastroenterol.
39, S111S124 (2005).
5. Lefebvre, P., Cariou, B., Lien, F., Kuipers, F.
& Staels, B. Role of bile acids and bile acid
receptors in metabolic regulation. Physiol. Rev.
89, 147191 (2009).
6. Brufau, G., Groen, A.K. & Kuipers, F. Reverse
cholesterol transport revisited: contribution of
biliary versus intestinal cholesterol excretion.
Arterioscler. Thromb. Vasc. Biol. 31, 17261733
(2011).
7. Oude Elferink, R.P., Frijters, C.M., Paulusma, C.
& Groen, A.K. Regulation of canalicular transport
activities. J.Hepatol. 24 (Suppl.1), 9499 (1996).
8. Verkade, H.J., Vonk, R.J. & Kuipers, F. New
insights into the mechanism of bile acid-
induced biliary lipid secretion. Hepatology 21,
11741189 (1995).
9. Parks, D.J. etal. Bile acids: natural ligands
for an orphan nuclear receptor. Science 284,
13651368 (1999).
10. Makishima, M. etal. Identification of a nuclear
receptor for bile acids. Science 284, 13621365
(1999).
11. Wang, H., Chen, J., Hollister, K., Sowers, L.C. &
Forman, B.M. Endogenous bile acids are ligands
for the nuclear receptor FXR/BAR. Mol. Cell 3,
543553 (1999).
12. Halilbasic, E., Claudel, T. & Trauner, M. Bile acid
transporters and regulatory nuclear receptors in
the liver and beyond. J.Hepatol. 58, 155168
(2013).
13. Sommer, F. & Backhed, F. The gut microbiota
masters of host development and physiology.
Nat. Rev. Microbiol. 11, 227238 (2013).
14. Backhed, F. Host responses to the human
microbiome. Nutr. Rev. 70 (Suppl.1), S14S17
(2012).
15. Karlsson, F.H. etal. Gut metagenome in
European women with normal, impaired and
diabetic glucose control. Nature 498, 99103
(2013).
16. Swann, J.R. etal. Systemic gut microbial
modulation of bile acid metabolism in host
tissue compartments. Proc. Natl Acad. Sci. USA
108 (Suppl.1), 45234530 (2011).
17. Sayin, S.I. etal. Gut microbiota regulates bile
acid metabolism by reducing the levels of
tauro--muricholic acid, a naturally occurring
FXRantagonist. Cell Metab. 17, 225235
(2013).
18. Li, F. etal. Microbiome remodelling leads to
inhibition of intestinal farnesoidX receptor
signalling and decreased obesity. Nat. Commun.
4, 2384 (2013).
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | ENDOCRINOLOGY ADVANCE ONLINE PUBLICATION | 9
19. Hofmann, A.F. & Eckmann, L. How bile acids
confer gut mucosal protection against bacteria.
Proc. Natl Acad. Sci. USA 103, 43334334
(2006).
20. Staels, B. & Kuipers, F. Bile acid sequestrants
and the treatment of type2 diabetes mellitus.
Drugs 67, 13831392 (2007).
21. Kir, S., Kliewer, S.A. & Mangelsdorf, D.J. Roles
of FGF19 in liver metabolism. Cold Spring Harb.
Symp. Quant. Biol. 76, 139144 (2011).
22. Potthoff, M.J. etal. FGF15/19 regulates
hepatic glucose metabolism by inhibiting the
CREB-PGC-1 pathway. Cell Metab. 13, 729738
(2011).
23. Kir, S. etal. FGF19 as a postprandial, insulin-
independent activator of hepatic protein and
glycogen synthesis. Science 331, 16211624
(2011).
24. Potthoff, M.J. etal. FGF21 induces PGC-1 and
regulates carbohydrate and fatty acid metabolism
during the adaptive starvation response. Proc.
Natl Acad. Sci. USA 106, 1085310858 (2009).
25. Maruyama, T. etal. Identification of membrane-
type receptor for bile acids (M-BAR). Biochem.
Biophys. Res. Commun. 298, 714719 (2002).
26. Kawamata, Y. etal. A Gprotein-coupled receptor
responsive to bile acids. J.Biol. Chem. 278,
94359440 (2003).
27. de Aguiar Vallim, T.Q., Tarling, E.J. &
Edwards,P.A. Pleiotropic roles of bile acids in
metabolism. Cell Metab. 17, 657669 (2013).
28. Pols, T.W., Noriega, L.G., Nomura, M., Auwerx, J.
& Schoonjans, K. The bile acid membrane
receptor TGR5: a valuable metabolic target.
Dig.Dis. 29, 3744 (2011).
29. Keely, S.J. Missing link identified: GpBAR1 is a
neuronal bile acid receptor. Neurogastroenterol.
Motil. 22, 711717 (2010).
30. Keitel, V. & Haussinger, D. Perspective: TGR5
(Gpbar-1) in liver physiology and disease. Clin.
Res. Hepatol. Gastroenterol. 36, 412419 (2012).
31. Thomas, C. etal. TGR5-mediated bile acid
sensing controls glucose homeostasis.
CellMetab. 10, 167177 (2009).
32. Makishima, M. etal. VitaminD receptor as an
intestinal bile acid sensor. Science 296,
13131316 (2002).
33. Germain, P., Staels, B., Dacquet, C.,
Spedding,M. & Laudet, V. Overview of
nomenclature of nuclear receptors. Pharmacol.
Rev. 58, 685704 (2006).
34. Kemper, J.K. Regulation of FXR transcriptional
activity in health and disease: Emerging roles
of FXR cofactors and post-translational
modifications. Biochim. Biophys. Acta 1812,
842850 (2011).
35. Fiorucci, S., Mencarelli, A., Distrutti, E.,
Palladino, G. & Cipriani, S. Targetting
farnesoid-X-receptor: from medicinal chemistry
to disease treatment. Curr. Med. Chem. 17,
139159 (2010).
36. Zhang, Y. & Edwards, P.A. FXR signaling in
metabolic disease. FEBS Lett. 582, 1018
(2008).
37. Thomas, A.M. etal. Hepatocyte nuclear factor4
and farnesoidX receptor co-regulates gene
transcription in mouse livers on a genome-wide
scale. Pharm. Res. 30, 21882198 (2013).
38. Lee, J. etal. Genomic analysis of hepatic
farnesoid X receptor binding sites reveals
altered binding in obesity and direct gene
repression by farnesoidX receptor in mice.
Hepatology 56, 108117 (2012).
39. Zhang, Y., Hagedorn, C.H. & Wang, L. Role of
nuclear receptor SHP in metabolism and cancer.
Biochim. Biophys. Acta 1812, 893908 (2011).
40. Zhang, Y., Kast-Woelbern, H.R. & Edwards, P.A.
Natural structural variants of the nuclear
receptor farnesoidX receptor affect
transcriptional activation. J.Biol. Chem. 278,
104110 (2003).
41. Huber, R.M. etal. Generation of multiple
farnesoid-X-receptor isoforms through the use of
alternative promoters. Gene 290, 3543 (2002).
42. Cariou, B. etal. The farnesoidX receptor
modulates adiposity and peripheral insulin
sensitivity in mice. J.Biol. Chem. 281,
1103911049 (2006).
43. Schote, A.B., Turner, J.D., Schiltz, J.
& Muller,C.P. Nuclear receptors in human
immune cells: expression and correlations.
Mol.Immunol. 44, 14361445 (2007).
44. Rizzo, G. etal. The farnesoidX receptor
promotes adipocyte differentiation and regulates
adipose cell function invivo. Mol. Pharmacol. 70,
11641173 (2006).
45. He, F. etal. Downregulation of endothelin-1 by
farnesoidX receptor in vascular endothelial
cells. Circ. Res. 98, 192199 (2006).
46. Nishimura, M., Naito, S. & Yokoi, T. Tissue-
specific mRNA expression profiles of human
nuclear receptor subfamilies. Drug Metab.
Pharmacokinet. 19, 135149 (2004).
47. Bishop-Bailey, D., Walsh, D.T. & Warner, T.D.
Expression and activation of the farnesoidX
receptor in the vasculature. Proc. Natl Acad. Sci.
USA 101, 36683673 (2004).
48. Abdelkarim, M. etal. The farnesoidX receptor
regulates adipocyte differentiation and function
by promoting peroxisome proliferator-activated
receptor-gamma and interfering with the
Wnt/-catenin pathways. J.Biol. Chem. 285,
3675936767 (2010).
49. Prawitt, J. etal. FarnesoidX receptor deficiency
improves glucose homeostasis in mouse
models of obesity. Diabetes 60, 18611871
(2011).
50. Zhang, Y. etal. Loss of FXR protects against
diet-induced obesity and accelerates liver
carcinogenesis in ob/ob mice. Mol. Endocrinol.
26, 272280 (2012).
51. Prawitt, J., Caron, S. & Staels, B. Bile acid
metabolism and the pathogenesis of type2
diabetes. Curr. Diab Rep. 11, 160166 (2011).
52. Bjursell, M. etal. Ageing Fxr deficient mice
develop increased energy expenditure,
improved glucose control and liver damage
resembling NASH. PLoS ONE 8, e64721
(2013).
53. Thomas, C., Pellicciari, R., Pruzanski, M.,
Auwerx,J. & Schoonjans, K. Targeting bile-acid
signalling for metabolic diseases. Nat. Rev. Drug
Discov. 7, 678693 (2008).
54. Haeusler, R.A., Pratt-Hyatt, M., Welch, C.L.,
Klaassen, C.D. & Accili, D. Impaired generation
of 12-hydroxylated bile acids links hepatic
insulin signaling with dyslipidemia. Cell Metab.
15, 6574 (2012).
55. Hu, X., Bonde, Y., Eggertsen, G. & Rudling, M.
Muricholic bile acids are potent regulators of
bile acid synthesis via a positive feedback
mechanism. J.Intern. Med. 275, 2738
(2014).
56. Bisschop, P.H. etal. Low-fat, high-carbohydrate
and high-fat, low-carbohydrate diets decrease
primary bile acid synthesis in humans.
Am.J.Clin. Nutr. 79, 570576 (2004).
57. Jonkers, I.J. etal. Fish oil increases bile
acid synthesis in male patients with
hypertriglyceridemia. J.Nutr. 136, 987991
(2006).
58. Duran-Sandoval, D. etal. Glucose regulates the
expression of the farnesoidX receptor in liver.
Diabetes 53, 890898 (2004).
59. Gineste, R. etal. Phosphorylation of farnesoidX
receptor by protein kinaseC promotes its
transcriptional activity. Mol. Endocrinol. 22,
24332447 (2008).
60. Berrabah, W. etal. The glucose sensing
O-GlcNacylation pathway regulates the nuclear
bile acid receptor FXR. Hepatology (2013).
61. Kemper, J.K. etal. FXR acetylation is normally
dynamically regulated by p300 and SIRT1 but
constitutively elevated in metabolic disease
states. Cell Metab. 10, 392404 (2009).
62. Inagaki, T. etal. Fibroblast growth factor15
functions as an enterohepatic signal to regulate
bile acid homeostasis. Cell Metab. 2, 217225
(2005).
63. Schmidt, D.R. etal. Regulation of bile acid
synthesis by fat-soluble vitaminsA and D.
J.Biol. Chem. 285, 1448614494 (2010).
64. Vergnes, L., Lee, J.M., Chin, R.G., Auwerx, J.
& Reue, K. Diet1 functions in the FGF15/19
enterohepatic signaling axis to modulate bile
acid and lipid levels. Cell Metab. 17, 916928
(2013).
65. Kurosu, H. etal. Tissue-specific expression
of -Klotho and fibroblast growth factor (FGF)
receptor isoforms determines metabolic activity
of FGF19 and FGF21. J.Biol. Chem. 282,
2668726695 (2007).
66. Boulias, K. etal. Regulation of hepatic
metabolic pathways by the orphan nuclear
receptor SHP. EMBO J. 24, 26242633
(2005).
67. Lundasen, T., Galman, C., Angelin, B. &
Rudling,M. Circulating intestinal fibroblast
growth factor19 has a pronounced diurnal
variation and modulates hepatic bile acid
synthesis in man. J.Intern. Med. 260, 530536
(2006).
68. Jones, S.A. Physiology of FGF15/19. Adv. Exp.
Med. Biol. 728, 171182 (2012).
69. Cicione, C., Degirolamo, C. & Moschetta, A.
Emerging role of fibroblast growth factors15/19
and 21 as metabolic integrators in the liver.
Hepatology 56, 24042411 (2012).
70. Angelin, B., Larsson, T.E. & Rudling, M.
Circulating fibroblast growth factors as
metabolic regulatorsa critical appraisal.
Cell. Metab. 16, 693705 (2012).
71. Dong, X. etal. Irs1 and Irs2 signaling is
essential for hepatic glucose homeostasis and
systemic growth. J.Clin. Invest. 116, 101114
(2006).
72. Fang, Q. etal. Serum fibroblast growth factor19
levels are decreased in Chinese subjects with
impaired fasting glucose and inversely
associated with fasting plasma glucose levels.
Diabetes Care 36, 28102814 (2013).
73. Barutcuoglu, B. etal. Fibroblast growth factor-19
levels in type2 diabetic patients with metabolic
syndrome. Ann. Clin. Lab. Sci. 41, 390396
(2011).
74. Keitel, V., Ullmer, C. & Haussinger, D. The
membrane-bound bile acid receptor TGR5
(Gpbar-1) is localized in the primary cilium of
cholangiocytes. Biol. Chem. 391, 785789
(2010).
75. Pellicciari, R. etal. Discovery of 6-ethyl-23(S)-
methylcholic acid (S-EMCA, INT-777) as a potent
and selective agonist for the TGR5 receptor, a
novel target for diabesity. J.Med. Chem. 52,
79587961 (2009).
76. Watanabe, M. etal. Bile acids induce energy
expenditure by promoting intracellular thyroid
hormone activation. Nature 439, 484489
(2006).
77. Watanabe, M. etal. Lowering bile acid pool size
with a synthetic farnesoidX receptor (FXR)
agonist induces obesity and diabetes through
reduced energy expenditure. J.Biol. Chem. 286,
2691326920 (2011).
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
10 | ADVANCE ONLINE PUBLICATION www.nature.com/nrendo
78. Watanabe, M. etal. Bile acid binding resin
improves metabolic control through the induction
of energy expenditure. PLoS ONE 7, e38286
(2012).
79. Maruyama, T. etal. Targeted disruption
of G protein-coupled bile acid receptor1
(Gpbar1/M-Bar) in mice. J.Endocrinol. 191,
197205 (2006).
80. Sato, H. etal. Anti-hyperglycemic activity of a
TGR5 agonist isolated from Olea europaea.
Biochem. Biophys. Res. Commun. 362, 793798
(2007).
81. Svensson, P.A. etal. The TGR5 gene is
expressed in human subcutaneous adipose
tissue and is associated with obesity, weight
loss and resting metabolic rate. Biochem.
Biophys. Res. Commun. 433, 563566 (2013).
82. Patti, M.E. etal. Serum bile acids are higher in
humans with prior gastric bypass: potential
contribution to improved glucose and lipid
metabolism. Obesity (Silver Spring) 17,
16711677 (2009).
83. Kohli, R. etal. Weight loss induced by Roux-en-Y
gastric bypass but not laparoscopic adjustable
gastric banding increases circulating bile acids.
J.Clin. Endocrinol. Metab. 98, E708E712 (2013).
84. Steinert, R.E. etal. Bile acids and gut peptide
secretion after bariatric surgery: a 1-year
prospective randomized pilot trial. Obesity
(SilverSpring) 21, E660E668 (2013).
85. Brufau, G. etal. Plasma bile acids are not
associated with energy metabolism in humans.
Nutr. Metab. (Lond.) 7, 73 (2010).
86. Ockenga, J. etal. Plasma bile acids are
associated with energy expenditure and thyroid
function in humans. J.Clin. Endocrinol. Metab.
97, 535542 (2012).
87. Jansen, P.L. etal. Alterations of hormonally
active fibroblast growth factors after Roux-en-Y
gastric bypass surgery. Dig. Dis. 29, 4851
(2011).
88. Gerhard, G.S. etal. A role for fibroblast growth
factor 19 and bile acids in diabetes remission
after Roux-en-Y gastric bypass. Diabetes Care
36, 18591864 (2013).
89. Pournaras, D.J. etal. The role of bile after
Roux-en-Y gastric bypass in promoting weight
loss and improving glycaemic control.
Endocrinology 153, 36133619 (2012).
90. Potthoff, M.J., Kliewer, S.A. & Mangelsdorf, D.J.
Endocrine fibroblast growth factors15/19 and
21: from feast to famine. Genes Dev. 26,
312324 (2012).
91. Morton, G.J. etal. FGF19 action in the brain
induces insulin-independent glucose lowering.
J.Clin. Invest. 123, 47994808 (2013).
92. Holst, J.J. & McGill, M.A. Potential new
approaches to modifying intestinal GLP-1
secretion in patients with type2 diabetes
mellitus: focus on bile acid sequestrants.
Clin.Drug Investig. 32, 114 (2012).
93. Holst, J.J. Enteroendocrine secretion of gut
hormones in diabetes, obesity and after bariatric
surgery. Curr. Opin. Pharmacol. 13, 983988
(2013).
94. Shah, M. etal. Contribution of endogenous
glucagon-like peptide-1 to glucose metabolism
after Roux-en-Y gastric bypass. Diabetes 63,
483493 (2014).
95. Claudel, T., Sturm, E., Kuipers, F. & Staels, B. The
farnesoid X receptor: a novel drug target? Expert
Opin. Investig. Drugs 13, 11351148 (2004).
96. Fiorucci, S., Mencarelli, A., Distrutti, E. &
Zampella, A. Farnesoid X receptor: from
medicinal chemistry to clinical applications.
Future Med. Chem. 4, 877891 (2012).
97. Porez, G., Prawitt, J., Gross, B. & Staels, B. Bile
acid receptors as targets for the treatment of
dyslipidemia and cardiovascular disease. J.Lipid
Res. 53, 17231737 (2012).
98. Schaap, F.G., Trauner, M. & Jansen, P.L. Bile
acid receptors as targets for drug development.
Nat. Rev. Gastroenterol. Hepatol. 11, 5567
(2014).
99. Halilbasic, E., Baghdasaryan, A. & Trauner, M.
Nuclear receptors as drug targets in cholestatic
liver diseases. Clin. Liver Dis. 17, 161189
(2013).
100. Trauner, M. etal. Targeting nuclear bile acid
receptors for liver disease. Dig. Dis. 29, 98102
(2011).
101. Chiang, J.Y. Bile acid metabolism and signaling.
Compr. Physiol. 3, 11911212 (2013).
102. Li, T. & Chiang, J.Y. Nuclear receptors in bile acid
metabolism. Drug Metab. Rev. 45, 145155
(2013).
103. Mudaliar, S. etal. Efficacy and safety of the
farnesoidX receptor agonist obeticholic acid in
patients with type2 diabetes and nonalcoholic
fatty liver disease. Gastroenterology 145,
57482.e1 (2013).
104. Reasner, C.A. Reducing cardiovascular
complications of type2 diabetes by targeting
multiple risk factors. J.Cardiovasc. Pharmacol.
52, 136144 (2008).
105. Robinson, J.G., Wang, S., Smith, B.J. &
Jacobson, T.A. Meta-analysis of the relationship
between non-high-density lipoprotein cholesterol
reduction and coronary heart disease risk. J.Am.
Coll. Cardiol. 53, 316322 (2009).
106. Garg, A. & Grundy, S.M. Cholestyramine therapy
for dyslipidemia in non-insulin-dependent
diabetes mellitus. A short-term, double-blind,
crossover trial. Ann. Intern. Med. 121, 416422
(1994).
107. Bays, H.E., Goldberg, R.B., Truitt, K.E. &
Jones,M.R. Colesevelam hydrochloride therapy
in patients with type2 diabetes mellitus treated
with metformin: glucose and lipid effects. Arch.
Intern. Med. 168, 19751983 (2008).
108. Fonseca, V.A., Rosenstock, J., Wang, A.C.,
Truitt,K.E. & Jones, M.R. Colesevelam HCl
improves glycemic control and reduces LDL
cholesterol in patients with inadequately
controlled type2 diabetes on sulfonylurea-based
therapy. Diabetes Care 31, 14791484 (2008).
109. Goldberg, R.B., Fonseca, V.A., Truitt, K.E. &
Jones, M.R. Efficacy and safety of colesevelam
in patients with type2 diabetes mellitus and
inadequate glycemic control receiving insulin-
based therapy. Arch. Intern. Med. 168,
15311540 (2008).
110. Rosenstock, J. etal. Initial combination
therapy with metformin and colesevelam for
achievement of glycemic and lipid goals in early
type2 diabetes. Endocr. Pract. 16, 629640
(2010).
111. Schwartz, S.L. etal. The effect of colesevelam
hydrochloride on insulin sensitivity and
secretion in patients with type2 diabetes:
apilot study. Metab. Syndr. Relat. Disord. 8,
179188 (2010).
112. Rosenson, R.S., Abby, S.L. & Jones, M.R.
Colesevelam HCl effects on atherogenic
lipoprotein subclasses in subjects with type2
diabetes. Atherosclerosis 204, 342344 (2009).
113. Zieve, F.J., Kalin, M.F., Schwartz, S.L.,
Jones,M.R. & Bailey, W.L. Results of the
glucose-lowering effect of WelChol study
(GLOWS): a randomized, double-blind, placebo-
controlled pilot study evaluating the effect of
colesevelam hydrochloride on glycemic control
in subjects with type2 diabetes. Clin. Ther. 29,
7483 (2007).
114. Ooi, C.P. & Loke, S.C. Colesevelam for type2
diabetes mellitus. Cochrane Database of
Systematic Reviews, Issue 12. Art. No.:
CD009361 http://dx.doi.org/ 10.1002/
14651858.CD009361.pub2.
115. Brufau, G. etal. Improved glycemic control
with colesevelam treatment in patients with
type2 diabetes is not directly associated with
changes in bile acid metabolism. Hepatology 52,
14551464 (2010).
116. Suhre, K. etal. Metabolic footprint of diabetes:
amultiplatform metabolomics study in an
epidemiological setting. PLoS ONE 5, e13953
(2010).
117. Bennion, L.J. & Grundy, S.M. Effects of
diabetes mellitus on cholesterol metabolism in
man. N.Engl. J.Med. 296, 13651371 (1977).
118. de Leon, M.P., Ferenderes, R. & Carulli, N.
Bilelipid composition and bile acid pool size in
diabetes. Am. J.Dig. Dis. 23, 710716 (1978).
119. Abrams, J.J., Ginsberg, H. & Grundy, S.M.
Metabolism of cholesterol and plasma
triglycerides in nonketotic diabetes mellitus.
Diabetes 31, 903910 (1982).
120. Haber, G.B. & Heaton, K.W. Lipid composition
of bile in diabetics and obesity-matched
controls. Gut 20, 518522 (1979).
121. Andersen, E., Karlaganis, G. & Sjovall, J. Altered
bile acid profiles in duodenal bile and urine in
diabetic subjects. Eur. J.Clin. Invest. 18,
166172 (1988).
122. Beysen, C. etal. Effect of bile acid sequestrants
on glucose metabolism, hepatic denovo
lipogenesis, and cholesterol and bile acid
kinetics in type2 diabetes: a randomised
controlled study. Diabetologia 55, 432442
(2012).
123. Shang, Q., Saumoy, M., Holst, J.J., Salen, G. &
Xu, G. Colesevelam improves insulin resistance
in a diet-induced obesity (F-DIO) rat model by
increasing the release of GLP-1. Am. J.Physiol.
Gastrointest. Liver Physiol. 298, G419G424
(2010).
124. Smushkin, G. etal. The effect of a bile acid
sequestrant on glucose metabolism in subjects
with type2 diabetes. Diabetes 62, 10941101
(2013).
125. Herrema, H. etal. Bile salt sequestration
induces hepatic denovo lipogenesis through
farnesoidX receptor- and liverX receptor
-controlled metabolic pathways in mice.
Hepatology 51, 806816 (2010).
126. Meissner, M. etal. Bile acid sequestration
reduces plasma glucose levels in db/db mice
byincreasing its metabolic clearance rate.
PLoSONE 6, e24564 (2011).
127. Hofmann, A.F. Bile acid sequestrants improve
glycemic control in type2 diabetes: a proposed
mechanism implicating glucagon-like peptide1
release. Hepatology 53, 1784 (2011).
128. Potthoff, M.J. etal. Colesevelam suppresses
hepatic glycogenolysis by TGR5-mediated
induction of GLP-1 action in DIO mice. Am.
J.Physiol. Gastrointest. Liver Physiol. 304,
G371G380 (2013).
129. Wu, T. etal. Effects of rectal administration of
taurocholic acid on glucagon-like peptide-1 and
peptideYY secretion in healthy humans.
Diabetes Obes. Metab. 15, 474477 (2013).
130. Lundasen, T. etal. Inhibition of intestinal bile acid
transporter Slc10a2 improves triglyceride
metabolism and normalizes elevated plasma
glucose levels in mice. PLoS ONE 7, e37787
(2012).
131. Kharitonenkov, A. etal. FGF-21 as a novel
metabolic regulator. J.Clin. Invest. 115,
16271635 (2005).
132. Coskun, T. etal. Fibroblast growth factor21
corrects obesity in mice. Endocrinology 149,
60186027 (2008).
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
NATURE REVIEWS | ENDOCRINOLOGY ADVANCE ONLINE PUBLICATION | 11
133. Xu, J. etal. Fibroblast growth factor21 reverses
hepatic steatosis, increases energy expenditure,
and improves insulin sensitivity in diet-induced
obese mice. Diabetes 58, 250259 (2009).
134. Brestoff, J.R. & Artis, D. Commensal bacteria at
the interface of host metabolism and the immune
system. Nat. Immunol. 14, 676684 (2013).
135. Papacleovoulou, G. etal. Maternal cholestasis
during pregnancy programs metabolic disease
in offspring. J.Clin. Invest. 123, 31723181
(2013).
136. Bochkis, I.M., Shin, S. & Kaestner, K.H. Bile
acid-induced inflammatory signaling in mice
lacking Foxa2 in the liver leads to activation
of mTOR and age-onset obesity. Mol. Metab. 2,
447456 (2013).
137. Russell, D.W. The enzymes, regulation, and
genetics of bile acid synthesis. Annu. Rev.
Biochem. 72, 137174 (2003).
138. Russell, D.W. Fifty years of advances in bile
acid synthesis and metabolism. J.Lipid Res.
50(Suppl.), S120S125 (2009).
Author contributions
F.K. researched the data for the article, provided
substantial contribution to discussions of the
content, contributed equally to writing the article and
reviewed and/or edited the manuscript before
submission. V.W.B. researched the data for the article
and reviewed and/or edited the manuscript before
submission. A.K.G. provided substantial contribution
to discussions of the content, contributed equally to
writing the article and reviewed and/or edited the
manuscript before submission.
REVIEWS
2014 Macmillan Publishers Limited. All rights reserved
You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Benefits of Yoga From HEAD To TOE (Based On Scientific Research)Document38 pagesBenefits of Yoga From HEAD To TOE (Based On Scientific Research)Ajay LochunNo ratings yet
- DiabetesDocument1 pageDiabetesJobelle Rodriguez BernabeNo ratings yet
- Calcium LieDocument14 pagesCalcium Liesusan64100% (4)
- Medical Hydrology and Balneology - Environmental AspectsDocument464 pagesMedical Hydrology and Balneology - Environmental Aspectse-bas-ti-necu-reciNo ratings yet
- Diabetes MellitusDocument64 pagesDiabetes MellitusCris Tine67% (6)
- Unit 5 Part 2 InsulinDocument68 pagesUnit 5 Part 2 InsulinKhairunnisa Loqman100% (1)
- Purslane Portulaca Oleracea Seed Consumption and ADocument11 pagesPurslane Portulaca Oleracea Seed Consumption and Alucaste50No ratings yet
- QuotesDocument41 pagesQuotesTrishenth FonsekaNo ratings yet
- Fitness and Health 2015Document6 pagesFitness and Health 2015cn_cadillacmiNo ratings yet
- The Quiescent Benefits and Drawbacks of Coffee IntakeDocument6 pagesThe Quiescent Benefits and Drawbacks of Coffee IntakeVikram Singh ChauhanNo ratings yet
- Galvus (Vildagliptin) : How Does It Work?Document5 pagesGalvus (Vildagliptin) : How Does It Work?Radhakrishna KurupNo ratings yet
- Disease Affecting PregnancyDocument3 pagesDisease Affecting PregnancyEmman Acosta DomingcilNo ratings yet
- Philippine Diabetes Mellitus Prevention and Control Program - Odita and RegundaDocument19 pagesPhilippine Diabetes Mellitus Prevention and Control Program - Odita and Regundakoala100% (1)
- Obesity TOGDocument7 pagesObesity TOGprincessmeleana64990% (1)
- Health History Format BlankDocument32 pagesHealth History Format BlankRich-Anne LagarasNo ratings yet
- Glycemic IndexDocument5 pagesGlycemic IndexftmtanNo ratings yet
- Soapi 1Document11 pagesSoapi 1api-330084238No ratings yet
- E147 Full PDFDocument21 pagesE147 Full PDFcahyatiNo ratings yet
- Health Teaching Plan Area: Barangay Balong Bato San Juan City Topic: Diet For Hypertension and DiabetesDocument5 pagesHealth Teaching Plan Area: Barangay Balong Bato San Juan City Topic: Diet For Hypertension and DiabetesGlaizalyn Fabella TagoonNo ratings yet
- (Churchill Pocketbooks) Sujoy Ghosh, Andrew Collier-Churchill's Pocketbook of Diabetes-Churchill Livingstone (2012)Document343 pages(Churchill Pocketbooks) Sujoy Ghosh, Andrew Collier-Churchill's Pocketbook of Diabetes-Churchill Livingstone (2012)Kirin Tor100% (1)
- MOH, DHA and Some HAAD 2017: This Question Shared in Whatapp GroupDocument32 pagesMOH, DHA and Some HAAD 2017: This Question Shared in Whatapp GroupshahzadNo ratings yet
- GDMDocument38 pagesGDMAbhishiktaAbhi100% (1)
- Assessment of Insulin Resistance by A 13C Glucose Breath TestDocument26 pagesAssessment of Insulin Resistance by A 13C Glucose Breath TestSuppiah AnarsalamNo ratings yet
- Low Carb Diet For Weight Loss and Diabetes - Unwin 2014 PDFDocument4 pagesLow Carb Diet For Weight Loss and Diabetes - Unwin 2014 PDFPaul MayNo ratings yet
- Diet Plan PDFDocument9 pagesDiet Plan PDFComet ShopNo ratings yet
- Does Family History of Obesity, Cardiovascular, and Metabolic Diseases Influence Onset and Severity of Childhood ObesityDocument6 pagesDoes Family History of Obesity, Cardiovascular, and Metabolic Diseases Influence Onset and Severity of Childhood ObesityTony Miguel Saba SabaNo ratings yet
- Lecture 32 - Nutritional DisordersDocument43 pagesLecture 32 - Nutritional Disordersapi-3703352100% (3)
- KNH 411 - Case Study 22Document17 pagesKNH 411 - Case Study 22api-301118772100% (3)
- Endocrine Medical Transcription SampleDocument2 pagesEndocrine Medical Transcription SampleMarisol Jane JomayaNo ratings yet